Best known for his viral comedy sketches and no-nonsense ‘Mum’ character, Richard is encouraging his fans to swap laughter for legwork in support of breast cancer research.
The social media star is supporting the challenge in memory of his mum, who sadly lost her life to cancer in 2014. Richard said:
Comedy is about bringing people together, and this challenge is no different. Cancer affects so many of us, either personally or through someone we love. I’m supporting this campaign for everyone whose lives have been impacted by this devastating disease.
Through his involvement, Richard hopes to inspire his followers and beyond to embrace healthier lifestyles that reduce cancer risk, while also fundraising for life-changing research.
In February, Richard will release a video featuring his ‘Mum’ character – showing support for the charity and encouraging fans and fellow creators to donate, share, and get involved with World Cancer Research Fund.
Reflecting on his much-loved character, Richard shared:
My mum was quite a character herself! She’s the inspiration behind ‘Mum’, and I’m proud to honour her memory in this way.
Funds raised from the challenge will be used to support the CANDO project – a five-year research programme at the University of Southampton exploring how body composition affects breast cancer treatment outcomes and side effects.
Ultimately, this research hopes to find kinder, more effective treatments for breast cancer patients.
Rachael Hutson, CEO at World Cancer Research Fund, commented:
On social media, he’s the ‘mum’ you should listen to and laugh along with! So, who better to raise awareness of cancer prevention and the importance of research in this area? We’re incredibly pleased that Richard is supporting this challenge. Around four in ten cancers are preventable, and with the help of Richard and everyone who donates, we’re taking important steps to reduce that risk.
You can follow Richard on TikTok at @richardfrankscomedy, and find out how to get involved with the challenge below:
More about Richard
Richard Franks is a comedian and writer who rose to prominence on TikTok and Instagram through short-form comedy videos, building an online community of over 1.3 million followers.
He is best known for his popular “Mum” sketches, portraying a sharp-witted, no-nonsense mother navigating everyday life.
Originally from High Wycombe and raised in Folkestone, Richard Franks began honing his comedy craft in 2011, before expanding his reach to social media in August 2020 with the launch of his channel @richardfrankscomedy.
Find out more about Richard: His work | Follow him on Instagram
We commend the UK Government for setting out an ambitious 10-year strategy with a strong focus on survival, innovation, and patient experience.
Yet the Plan misses a chance to put prevention front and centre, with stronger alcohol policy, breastfeeding protection, and a dedicated focus on the modifiable risk factors that drive cancer
A bold ambition on survival and care
We particularly welcome the Government’s bold target that 75% of people diagnosed with cancer from 2035 will be cancer-free or living well five years after diagnosis – a genuine step change in ambition. The Plan’s emphasis on earlier diagnosis, reducing emergency presentations, expanding evidence-based screening, and improving access to innovative treatments has the potential to deliver meaningful improvements for patients across England.
We also welcome commitments to improve patient experience and outcomes, including personalised care, better coordination, and stronger accountability for delivery through a reformed National Cancer Board.
Progress on prevention – but a missed opportunity to go further
We welcome the Plan’s commitments on cancer prevention, including action to crack down on the illegal use of sunbeds and harmful UV exposure, progress towards a smoke-free generation, and expanded access to HPV vaccination as part of the ambition to eliminate cervical cancer. These are important, evidence-based interventions that will prevent cancers and reduce future pressure on the health system.
However, prevention deserves greater prominence. New global evidence shows that up to four in ten cancers worldwide are linked to preventable causes. Tackling the lifestyle and environmental factors that increase cancer risk is one of the most effective and affordable ways to prevent cancer in the long term.
Crucially, modifiable risk factors are not evenly distributed. Tobacco use, harmful alcohol consumption, unhealthy diets and obesity disproportionately affect people in lower socio-economic groups, driving stark and persistent inequalities in cancer incidence, survival and mortality. Strong, population-level prevention policies are therefore essential not only to reduce cancer overall, but to narrow health inequalities and ensure the benefits of progress are shared fairly.
We believe the Plan would have benefitted from a dedicated chapter on prevention, helping to drive a necessary mindset shift and embed the principle that diet, alcohol, and breastfeeding policies are cancer policies.
Action on alcohol and breastfeeding is lacking
The Plan does not expansively build on the wider prevention measures announced in the Government’s 10 Year Health Plan, particularly in relation to alcohol policy. Alcohol remains a leading avoidable cause of cancer, yet the Plan does not commit to minimum unit pricing (MUP) or restrictions on alcohol advertising and marketing, including where it reaches children and young people – among the most effective and evidence-based tools for reducing population-level alcohol harm and cancer risk.
We also note the absence of strengthened action to protect breastfeeding, including full compliance with the International Code of Marketing of Breast-milk Substitutes. Breastfeeding reduces cancer risk for mothers and improves long-term health outcomes for children, and stronger implementation of the Code should form part of a comprehensive, life-course approach to cancer prevention.
Partnerships with food manufacturers must also be approached with caution, given past experience of policy dilution. Where voluntary approaches fall short, Government must not shy away from mandatory measures. Strong governance, transparency, and protection from undue commercial influence are essential to ensure prevention policies deliver for public health.
Biomedical innovation matters but it is not enough
We are pleased to see the Plan’s commitment to biomedical prevention, including continued rollout of the HPV vaccine, trials of preventative vaccines such as LungVax, and plans to accelerate uptake of GLP-1 medicines for those who clinically need them. These innovations are hugely important and represent real progress in reducing cancer risk and improving outcomes.
But vaccines and medicines alone are not sufficient. We must also tackle the environments that make us sick. We cannot continue to treat people only to send them back to the same food, alcohol, and physical environments that drove ill health in the first place. Population-level prevention policies remain essential to reducing cancer incidence at scale.
Crucially, prevention is not only about avoiding diagnosis. It also supports survival and quality of life, contributing directly to living well with and beyond cancer. Good nutrition, physical activity, and maintaining a healthy weight are fundamental to recovery, rehabilitation, and long-term wellbeing. Prevention and survivorship are not competing priorities – they are mutually reinforcing.
Digital innovation as a driver of prevention
We welcome the ambition to harness digital innovation through the NHS App. By 2028, the App will allow patients to manage screening invitations, appointments, treatment plans, and prehabilitation, with personalised prevention advice drawing on genomic, lifestyle, and wearable data.
This creates a major opportunity to establish the NHS App as a trusted, accessible source of cancer prevention information, supporting people to understand and act on behaviours that can influence cancer risk over their lifetime. We would welcome the opportunity to contribute evidence-based, tried and tested prevention resources, developed and evaluated for public audiences, to support this ambition and ensure alignment with the best available science.
Prehabilitation, rehabilitation and supportive oncology
We strongly welcome the Plan’s focus on prehabilitation, rehabilitation, and supportive oncology, including dietary and physical activity advice, psychological support, and acute oncology for those with more complex needs. The evidence is clear: these interventions improve treatment tolerance, recovery, and long-term outcomes. We believe the ambition should be for these services to be available to all patients, where appropriate, as standard.
Research and the cancer workforce
Research and the cancer workforce will be central to delivering the Plan’s ambitions. While we acknowledge the focus on accelerating clinical research and innovation, there is a clear opportunity to strengthen investment in cancer prevention research, including implementation research on modifiable risk factors. Healthcare professionals must also be supported with the time, training, and tools to deliver prevention, behaviour change, and survivorship support alongside treatment.
Children and young people
We welcome the Plan’s commitment to improving nutrition for children and young people undergoing cancer treatment in acute settings. Good nutrition is fundamental to treatment tolerance, recovery, and survival. We hope this approach will be extended to all patients, and that public procurement across health settings consistently meets the highest nutritional and sustainability standards through the upcoming NHS food standards review.
Matching survival ambition with prevention action
We welcome the ambition and scope of the National Cancer Plan. The integration of prehabilitation, rehabilitation, supportive oncology, digital innovation, and prevention advice into the cancer pathway is a significant step forward.
However, there remains a missed opportunity to embed prevention at the heart of the Plan, through stronger alcohol policy, breastfeeding protection, and a dedicated focus on the modifiable risk factors that drive cancer incidence.
A Plan that matches its ambition on survival with bold, population-level prevention action will reduce cancer incidence, improve outcomes, and deliver a financially sustainable cancer strategy for generations to come.
We stand ready to work with Government, healthcare professionals, and partners to help make this ambition a reality.
More policy-related news and blogs



It has long been established that junk food advertising drives consumption of unhealthy food and drink, shaping preferences from a young age and contributing to overweight and obesity.
The strength of the evidence base is perhaps best corroborated by the enormous advertising budgets of unhealthy food and drink companies. If advertising didn’t pay off, why would Coca-Cola allocate a whopping $5 billion to their worldwide advertising budget in 2024?
Restricting junk food advertising is therefore a powerful and proven public health measure. Yet, most recently, you may have seen measured responses from public health advocates in the UK, including World Cancer Research Fund, upon the introduction of long-awaited junk food advertising restrictions in January 2026.
Marketing regulations can underdeliver
The bottom line is that whilst the UK’s restrictions mark a step forward in protecting children’s health at a time when obesity rates continue to rise, they have been weakened and delayed by industry influence – most notably through the introduction of a sweeping brand exemption. This significantly undermines the policy in two key ways. First, it allows brands that are synonymous with foods high in fat, salt and sugar (HFSS) to continue being advertised – think the famous Golden Arches. Second, the lack of brand restrictions enables companies to promote entire HFSS product ranges, just not individual products. Ultimately this preserves brand visibility and influence while circumventing the spirit of the regulations.
The brand exemption is not the only weakness of the advertising restrictions. Work on this policy began as far back as 2018, and in the years since, the marketing landscape has evolved dramatically. Simply put, the regulations are not a match for the rapidly changing marketing landscape. For example, direct marketing channels, such as email and text messaging, remain unchecked, allowing unhealthy food and drink companies to continue targeting consumers.
The unseen cost of delays and dilution
The unfortunate tale of industry influence is not unique to the UK. Globally, efforts to curb the scourge of junk food on society are denied, diluted, derailed and delayed by industry.
Marketing restrictions are difficult to get over the line. In the UK, the policy was subject to five separate consultations and four delays to its rollout. That is an immense amount of government time, effort and resources. Moreover, the burden it places on the public health sector, which often operate under capacity constraints, must be acknowledged.
We also need to recognise that obesity, a key risk factor for cancer, is linked to deprivation. In many countries, those living in the most deprived areas are more likely to be living with obesity compared to those in the most affluent communities. Delays or failures to implement effective policies therefore disproportionately impact those who are already most vulnerable.
Industry opposition at full throttle
The resistance we see to advertising restrictions can partly be explained by the fact that marketing is not a peripheral commercial function. Instead, it sits at the very core of food and drink businesses, playing a pivotal role in building brand value, customer loyalty and long-term profitability.
Marketing restrictions are also unusually visible. Unlike reformulation targets or nutrient thresholds, which operate largely behind the scenes, advertising bans are immediately noticeable. They can also be drawn into wider debates around personal responsibility, censorship and creativity – making the more contested and politically charged. They tend to hit a nerve.
Recognition of these issues is not a justification for inaction. The reality is that companies by their very nature are required to innovate, and they can do so in a way that supports public health rather than undermining it.
Action must go beyond the status quo
Let’s be clear, no one is suggesting that junk food marketing restrictions alone will solve the obesity crisis. However, the version we’ve seen introduced in the UK will most certainly underdeliver, especially given the restrictions don’t sit within a broader framework of measures designed to improve the nation’s diet yet. Countries in Latin America, including Chile and Mexico, have taken more holistic approaches which embed marketing restrictions within a wider set of measures including mandatory warning labels and robust school food standards
But when governments introduce policies that appear ambitious on paper but lack the strength to deliver in practice, they risk entrenching the status quo while giving the impression of action. This pattern is not unique to food. Similar delays and dilutions are seen across alcohol, gambling and other health-harming industries, where commercial interests routinely take priority over public health.
Ultimately, the question is not what needs to be done, but what governments are willing to do to protect public health.
Related news and blogs



Today the UK Government published a long-awaited update to the Nutrient Profile Model (NPM) – a quiet but powerful public health tool that is central to cancer prevention and tackling diet-related diseases.
NPMs are used to assess how healthy foods are, classifying products as healthier or less healthy (often referred to as HFSS – high in fat, salt and sugar). While no system is perfect, the NPM is critical because it underpins food policy, determining which products are captured by regulation and which are allowed to escape it.
The UK’s existing junk food advertising and promotion restrictions are still based on the 2004 NPM. This means the effectiveness of these policies depends entirely on a model developed more than 20 years ago.
A robust, evidence-based NPM is essential to prevent unhealthy products continuing to fall through regulatory gaps. Since the original model was developed, the science on diet and health has moved on.
Obesity firmly established as major driver of cancer
In particular, evidence linking unhealthy diets, overweight and obesity, and cancer risk has grown substantially. Obesity is now firmly established as a major driver of cancer and one of the leading preventable causes of the disease in the UK and globally. If food policy is to meaningfully improve diets and reduce obesity-related cancer risk, it must be built on a credible, up-to-date NPM.
Importantly, the updated NPM will better reflect recommendations from the independent Scientific Advisory Committee on Nutrition (SACN) on free sugars and fibre, ensuring policy aligns with current scientific guidance.
We therefore warmly welcome today’s publication of the revised NPM, first consulted on in 2018. This is an important step forward. However, the updated NPM is not yet applied in policy.
The Government has committed to holding a public consultation in 2026 on applying the 2018 NPM to advertising and promotion restrictions. We stand ready to work with the UK Government at this next stage to ensure the NPM delivers real progress for cancer prevention and overall public health.
More policy-related news and blogs
World Cancer Research Fund – part of the World Cancer Research Fund network – welcomes many of the recommendations in the new US Dietary Guidelines for Americans that support healthier diets and reduce the burden of diet-related disease.
When it comes to cancer prevention, we have some concerns with the guidelines relating to alcohol and red and processed meat.
The strong emphasis on healthy dietary patterns, including increased consumption of fruits, vegetables and wholegrains, is very helpful – as are the recommendations to limit highly processed foods and products high in added sugars. The clear inclusion of plant-source protein foods – such as beans, lentils, nuts, seeds and soy – is also positive.
The guidance to drink mainly water and to avoid sugar-sweetened beverages and consume less alcohol is helpful, as we know there is no safe level of drinking alcohol when it comes to cancer prevention. Finally, we strongly welcome support for breastfeeding.
These Guidelines help to translate evidence into clear public advice and shape future policies. However, from a cancer prevention perspective, the Guidelines’ increased emphasis on animal-source proteins, and particularly the emphasis on red meat, is at odds with the scientific evidence linking higher intakes of red and processed meat to increased cancer risk.
Similarly, the promotion of whole-fat dairy raises concerns, given the potential contribution to excess weight gain. In light of such issues, we remain committed to informing the public with authoritative advice, which we develop based on the latest scientific evidence from leading researchers worldwide.
Below is a more detailed summary of the what the Guidelines mean for cancer prevention.
Important takeaways from the guidance
- Clear guidance is provided to prioritise whole foods and limit highly processed products, including advice to avoid salty and sweet packaged snacks and to favour nutrient-dense, home-prepared meals. This approach is closely aligned with our emphasis on limiting fast foods and processed foods high in fat, starches and sugars, and on reducing overall dietary energy density as a pathway to achieving a healthier body weight and lowering cancer risk.
- The Guidelines strengthen the stance on added sugars and sugar-sweetened beverages, including explicit recommendations to limit consumption of sugar-sweetened drinks and to limit added sugars at meals. This aligns well with our evidence of sugar intake as a contributor to excess weight gain and poorer overall diet quality.
- Plant foods remain important to the guidance, with daily targets for fruit and vegetable intake and a clear recommendation to prioritise fibre-rich whole grains. This maps directly onto our emphasis on dietary and lifestyle patterns and core cancer prevention recommendations.
- Breastfeeding is explicitly encouraged, with guidance to breastfeed exclusively for the first six months and to continue breastfeeding for two years or beyond. This is consistent with our recommendation that mothers breastfeed where possible and complements the focus on breast cancer prevention.
Important clarifications based on our global scientific research
- The Guidelines place a strong emphasis on increasing protein intake, explicitly including red meat and setting a higher quantitative protein target.
From a cancer prevention perspective, this emphasis would benefit from clearer direction to prioritise plant-based protein sources such as tofu, beans, lentils and other legumes, as well as nuts, seeds, fish and poultry, while reiterating World Cancer Research Fund guidance to limit red meat consumption and avoid processed meat altogether. - Furthermore, the Guidelines promote protein-rich foods, in relation to meat; specifically, meat with no or limited added sugars, refined starches or chemical additives is recommended. Avoidance of processed meat aligns with our recommendation to eat little, if any, processed meat based on strong evidence of an increased risk of colorectal cancer.
- While the Guidelines prioritise fibre-rich wholegrains, they do not have significant prominence in the new ‘Real Food’ pyramid, which undermines their importance.
- The Guidelines adopt a general recommendation to consume less alcohol. For cancer prevention, it is best not to drink alcohol at all, as there is no safe threshold of consumption for cancer risk for at least seven cancer types.
- The explicit endorsement of full-fat dairy, with guidance to consume three servings per day, warrants careful interpretation given its contribution to excess weight and some variation in evidence by cancer site. Framing dairy as one possible option, rather than a central or universal recommendation, may therefore be more appropriate.
- The Guidelines’ discussion of “healthy fats” includes foods such as butter and beef tallow, while still recommending that saturated fat remain below 10% of total energy intake.
This recommendation needs careful explanation because butter and beef tallow are high in saturated fat and can affect overall energy balance. Maintenance of a healthy weight is important, as overweight and obesity increase the risk of at least 13 cancers.
Three important policy implications for the future
- Affordability and access: Achieving the dietary pattern outlined in the guidelines will require targeted policy measures to improve the availability and affordability of fresh and whole foods. At present, such diets remain out of reach for many Americans, particularly those on lower incomes. Without significant structural interventions there is a risk that the guidelines may exacerbate existing health inequalities.
- Clarity and implementation: Greater clarity is needed on how “highly processed foods” are defined within the guidelines and how this definition will be operationalised. Clear definitions are essential to inform coherent policy action, regulation, monitoring and public communication.
- Policy alignment and delivery: It remains unclear whether new or strengthened policy measures will be introduced to support the recommended dietary changes, or how these guidelines will be embedded across food, agriculture, procurement and public health policies to enable meaningful implementation. In addition, the guidelines should also consider broader factors such as sustainability and planetary health.
Explore our research
More useful information
After years of delays, a law to ban ads for unhealthy food and drink before 9pm on TV and across online platforms, will start.
Commenting on the ban, Dr Giota Mitrou, Executive Director of Research and Science at World Cancer Research Fund (WCRF) International, said:
“Marketing is a well-established driver of consumption of unhealthy foods, and children – who are the primary targets of junk food advertising by large corporations – are particularly vulnerable. These long-awaited restrictions therefore mark an important step forward in protecting children’s health.
“However, we must recognise the fact that these measures have not only been severely delayed, but also significantly weakened by broad exemptions for brand advertising.
“The scale of childhood obesity crisis demands greater and more far-reaching action. The latest data shows that 10.5% of children in Reception and 22.2% of children in Year 6 are living with obesity, with prevalence more than double in the most deprived areas compared with the least deprived.
“The UK government must expand the range of products in scope of the ban, removing brand exemptions, and extend protections to the outdoor environment. We must not let large corporations’ water down and undermine efforts to give all children the healthiest start.
World Cancer Research Fund remains committed to working with the government to address obesity, which is a cause of at least at least 13 types of cancer.”
Delay to the junk food marketing restrictions
In 2020 – as part of its Obesity Strategy – the government under Boris Johnson promised to implement a ban on products that were high in fat, salt and sugar (HFSS) online and before 9pm on TV, saying it would come into force by 2023.
However, under pressure from industry, the enforcement was delayed while a further review was undertaken.
These delays mean that today’s implementation will be three years later than originally promised, and severely weakened.
Research has demonstrated that children eat significantly more calories in a day, after watching just 5 minutes of junk food advertising.
Building Momentum report
In 2020, World Cancer Research fund produced its Building Momentum report showing the lessons of implementing robust restrictions of food and non-alcoholic beverage marketing to children
More policy-related news and blogs
Understanding the origins of bowel cancer risk
Our funded research showed greater birthweight or body size during childhood, adolescence or young adulthood was linked with higher risk of bowel cancer in later life.
It was the first CUP Global review to analyse and judge all the research examining how factors such as weight, height and body size in early life relate to our risk of bowel cancer as we get older.
Brisk walking cold reduce your cancer risk
Our funded researchers published evidence that brisk walking is linked to a lower risk of 5 cancers, including anal, liver, small intestine, thyroid, and lung.
Smaller waist or more exercise? For cancer prevention, both is best
In the world’s first study looking at the effectiveness of combining maintaining a smaller waist with staying active, we found that only doing one is not enough to lower our risk of cancer.
The study found that people not meeting World Health Organization (WHO) guidelines on waist circumference are at 11% greater risk, even if they are physically active.
And people not meeting WHO guidelines for physical exercise are at 4% greater risk, even if “abdominally lean” (i.e. they have a smaller waist). Achieving neither means a 15% greater risk.
The simple rule that cuts cancer risk by 23%
We released a first-of-its-kind study into how the number of different food types consumed, measured as Dietary Species Richness (the number of species an individual consumes per year) affects the risk of developing gastrointestinal cancer.
The study found that individuals with the most diverse diets had a 23% lower risk of developing gastrointestinal cancers compared with those with the least variety. The risk decreased by 6% for every 10 extra species per year added to their diet.
The growing need for your support
Your generous donations have enabled us to fund 19 new research grants this year, worth a total of £5 million, bringing our network’s achievements over the last 20 years to more than 200 research grants awarded and over £50m invested in research overall.
Over the past year, 13 projects came to a close, delivering inspiring new findings. These completed studies explored many ways to prevent cancer, improve treatment, and support people living with and beyond the disease. They examined how factors like body weight, nutrition, inflammation, and even sleep patterns may influence cancer risk, treatment side effects, and recovery.
Some looked at how early-life infections, obesity, and physical activity can affect cancer risk later in life, while others tested promising treatments or searched for new ways to use cancer drugs. There were also studies researching how to help people living with and beyond cancer live healthier lives, from technology-based tools and personalised vitamin D supplements to culturally tailored support for Indigenous communities and families of children with cancer.
As the number of cancer diagnoses grows worldwide, research into cancer prevention is more vital than ever. Thanks to your continuing support, we can continue to fund novel and innovative research and push the boundaries of knowledge on cancer research so that fewer people die from a preventable cancer.

The original CMA study made 11 important recommendations to bring the UK closer in line with international standards, address high formula prices and tackle inappropriate marketing practices.
Crucially, these important recommendations by the CMA also serve to ensure that breastfeeding – which protects babies against overweight and obesity, and mothers against breast cancer – is not undermined.
The long-awaited response from the UK government and four nations sets out several positive steps. It is encouraging to see commitments to make information for parent’s clearer in retail settings, clarify what constitutes advertising and give families more flexible ways to pay for formula.
These actions are welcome, but ultimately addressing excessively high formula prices remains the most equitable and impactful way to support families – especially during a cost-of-living crisis.
We also welcome the government’s intention to explore recommendations that would extend advertising restrictions to follow-on formula and require manufacturers to clearly show on product labels that all formula meets nutritional requirements and avoid vague or misleading claims.
These measures are vital to ensure parents receive clear, unbiased information in all settings and that marketing practices are fair and transparent.
However, it is disappointing that some recommendations – such as introducing standardised packaging in hospitals and establishing a pre-approval process for labels – have not been taken forward at this stage.
We are also clear that relying on voluntary action from manufacturers is unlikely to deliver meaningful change in a market dominated by a few large companies. We hope the government keeps this under review and does not shy away from mandatory measures if needed in future.
Kate Oldridge-Turner, Head of Policy and Public Affairs, said:
‘Infant nutrition is a public health priority with lifelong implications, including for cancer risk. The government’s response is a positive step forward in improving information provided to families about breast milk substitutes for those who need them. We are keen to work with government to ensure that every family has access to affordable products and services they need to ensure the best start in life for their child – and that they are protected from insidious marketing practices that skew feeding choices.’

Get the latest Policy updates
Receive the latest on our databases, publications and how we’re getting involved in cancer prevention policy around the world
Latest news and blogs



January: Setting the scene for prevention
We started the year strongly with the launch of our Policy Blueprint for Cancer Prevention, our new flagship advocacy tool outlining a clear roadmap for policymakers to curb rising cancer rates through prevention. Bringing together evidence and policy guidance across diet, weight, breastfeeding, physical activity, and alcohol, the blueprint offers practical tools and factsheets to support healthier environments and reduce inequities.
It also highlights the wider co-benefits of prevention for resilient health systems, economies, and societies. Since launch, it has been downloaded 1433 times (and is our 5th most popular download) and presented at 2 conferences.
February: Taking international nutrition policy to UK Parliament

We participated in our first Obesity Health Alliance parliamentary event, meeting with the Minister for Prevention and 11 other Members of Parliament (MPs) to share our expertise in international nutrition policy.
We highlighted the link between obesity and cancer and the need for an integrated policy approach, as set out in our Policy Blueprint for Cancer Prevention.
We also shared best practice examples from other countries that the UK can learn from – critically demonstrating to MPs that it is possible for the UK to take meaningful action on obesity.
March: Welcoming new Policy Advisory Group members
Our Policy Advisory Group brings together leading policy experts from government, academia, and civil society around the world to guide WCRF’s efforts to turn evidence into action.
In March we officially welcomed four new members to the group: Dr Henry Li (UK), Dr Terry Slevin (Australia), Pubudu Sumanasekara (Sri Lanka), and Dr Si Thu Win Tin (Fiji) – expanding the group’s expertise to include more of our policy priority areas and increasing regional representation.
April: Making prevention central to England’s National Cancer Plan
Following the UK government’s World Cancer Day announcement of a new National Cancer Plan for England, we responded to the call for evidence with a clear message: prevention must be central.
Global reviews show most National Cancer Control Plans overlook prevention, and England must not repeat this mistake. Our submission therefore called for strong primary and tertiary prevention measures and bold action on modifiable risk factors such as alcohol and obesity.
Prevention remains the most sustainable and cost-effective way to reduce the growing cancer burden. We expect the National Cancer Plan for England to be published in early 2026.
May: Influencing global health for cancer prevention
In May, we attended the UN’s Multi-stakeholder Hearing in New York ahead of the 4th High-Level Meeting (HLM) on NCDs and mental health. We delivered a clear statement urging governments to prioritise cancer prevention through evidence-based, cost-effective policies.
We also launched our advocacy push around our HLM policy brief – calling for bold action on prevention, equity, and protection from industry interference – while meeting with key negotiating blocs.
We highlighted that around 40% of cancers are preventable by addressing modifiable risk factors. This engagement was a key moment in building momentum ahead of the Political Declaration negotiations later in the year.
June: Sparking a national conversation on alcohol and cancer

June was a highlight of our year as we marked Cancer Prevention Action Week (CPAW) in the UK, this time focusing on the little-known link between alcohol and cancer. Our bold campaign sparked a national conversation on alcohol consumption and raised awareness of the fact that it increases the risk of 7 cancers.
Working alongside more than 20 organisations and experts, we urged the government to implement a National Alcohol Strategy for England including evidenced-based policies such as minimum unit pricing, marketing restrictions and labelling.
We are thrilled that the government heeded one of our calls, with a commitment to introduce mandatory labelling.
July: Creating UK Parliamentary history
We also supported the first-ever UK Parliamentary debate on alcohol and cancer, which marked a historic moment in raising awareness of this long-overlooked cause of preventable cancer.
Led by Cat Smith MP, the cross-party discussion called for a comprehensive National Alcohol Strategy aligned with WHO ‘Best Buys’. Although the government ruled out a strategy, it did commit to mandatory alcohol labelling with health warnings and nutritional information – a welcome but partial step.
We’ve kept the pressure on alcohol policy since, with work on alcohol licensing, drink driving limits and the forthcoming consultation on labelling.
August: Presenting at the International Congress on Nutrition
We showcased our science and policy expertise on nutrition, cancer prevention and survivorship at the International Congress of Nutrition (ICN) at the end of August in Paris.
This included co-hosting a scientific symposium with Fédération Française de Nutrition (FFN) on our CUP Global Dietary and Lifestyle patterns report, as well as e-posters on our Policy Blueprint for Cancer Prevention and Policy recommendations to reduce the health impacts of alcohol.
September: Global Spotlight – UN High-Level Meeting on NCDs and Mental Health

After an intense year of global health activity, the 4th UN High-Level Meeting on NCDs and mental health took place on 25 September in New York. The week was packed with NCD-focused side events and bilateral meetings, where we advocated for stronger, bolder global action on NCDs.
Although the final Political Declaration fell short on ambition for prevention, it included important recognition of cancer and the vital role of quality research. Many heads of state and ministers expressed strong national commitments to tackling NCDs and mental health and emphasised the need for urgent, bold action.
October: The 5th European Code Against Cancer
In October, the 5th edition of the European Code Against Cancer was launched, summarising the most up-to-date knowledge of the preventable causes of cancer.
It includes a set of 14 recommendations to help prevent cancer for individuals, including tobacco smoking, overweight and obesity, unhealthy diet, and lack of physical activity.
We are very proud that our research on these risk factors helped shape these 14 evidence-based recommendations.
November: Connecting with global cancer leaders
We attended the World Cancer Leaders’ Summit, strengthening global partnerships and exploring new collaboration opportunities – including with Australian research leaders and partners from Hong Kong ahead of next year’s World Cancer Congress.
We also met with IARC as they prepare for their 60th anniversary and aligned with the Union for International Cancer Control on promoting the new World Cancer Declaration.
We ended the week in Melbourne visiting Cancer Council Victoria, meeting our grant holders and PhD students – an inspiring reminder of the global partnerships that power our mission to prevent cancer worldwide.
December: Making mandatory alcohol labelling a reality
After securing a major public health victory with the UK government’s commitment to introduce mandatory alcohol labels featuring health warnings and nutritional information, the team is now consulting international partners in countries where similar measures have been considered such as Ireland, South Korea and Norway, to inform our position.
The evidence is clear: cancer warnings are particularly effective in changing consumption behaviours and can help address low awareness of alcohol’s link to cancer. Throughout 2026 and beyond, we will be working to ensure that labels are protected from industry influence and implemented at pace – this is a public health imperative.
Coming up in 2026:
- Review of NOURISHING and MOVING frameworks and databases
- Expanded policy work on breastfeeding, infant nutrition and cancer
- Greater policy focus on cancer survival and adherence to our Cancer Prevention Recommendations
- Providing policy perspectives to new CUP Global reviews and recommendations – including Ultra-processed foods
- Presence at the World Cancer Congress 2026
Read our previous annual round-ups




Get the latest Policy updates
Receive the latest on our databases, publications and how we’re getting involved in cancer prevention policy around the world
Latest news and blogs
Ahead of the Budget, the Chancellor said it would deliver on the priorities of the British people to cut waiting lists, national debt and the cost of living.
In response to the Autumn Budget 2025, Kate Oldrige Turner, Head of Policy and Public Affairs at World Cancer Research Fund said:
“Almost half of cancer cases are preventable by addressing key risk factors such as obesity and alcohol, so we are pleased to see the UK Government take concrete steps on prevention in this Autumn Budget.
“The expansion of the UK’s world-leading levy on sugar-sweetened beverages to include milk-based drinks and plant-milk alternatives, alongside lowering the sugar threshold to 4.5g per 100ml, are particularly welcome measures. This will build on the immense success of the levy, which has reduced the average sugar content of drinks sold in the UK by almost half since it was introduced. Crucially, it will drive further reformulation and ensure that more drinks sold to consumers are healthier.
“We are also relieved that the Chancellor will raise alcohol duty in line with inflation. The World Health Organization has identified alcohol duty as one of the most effective ways to tackle alcohol-related harm, including alcohol-related cancers, so we are glad to see the UK Government take this forward.
As a research funder, we would have liked to see the important contribution of the life sciences sector acknowledged in the Chancellor’s speech. Continued support and investment in research are essential to advance our understanding of cancer prevention and survivorship.
To improve public health and reduce burden on the NHS, today’s measures must be the beginning – not the end – of a bold approach to prevention. With the National Cancer Plan for England expected early next year, the UK has a crucial opportunity to put prevention at the heart of its cancer strategy.
We look forward to working with the UK government to make prevention a reality – helping millions of people live free from the devastating effects of cancer.
Latest news and blogs
Donations from our fantastic supporters are smartly invested into the most impactful opportunities in science, guided by our wide network of independent leading experts.
Each year, millions of people hear the words “you have cancer” – and millions more are quietly edging towards a preventable diagnosis because of factors like diet, weight, inactivity or environmental exposures.
There’s a huge opportunity here: we know that 40% of cancer cases could be prevented. But there are still major gaps in the evidence that our latest round of awards will help to fill.
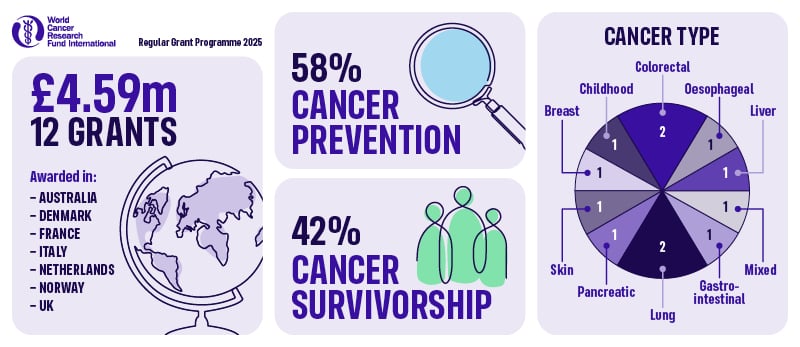
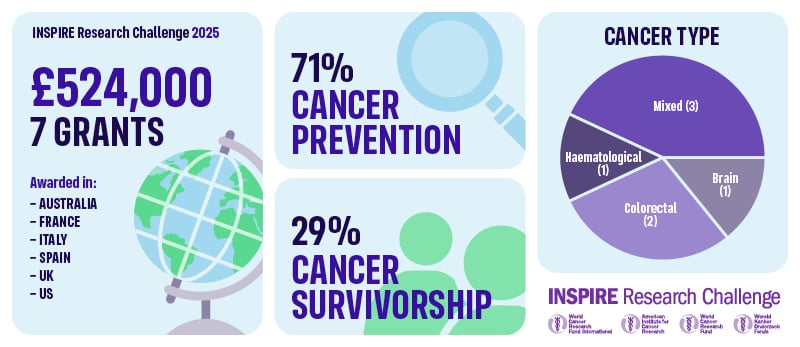
The three charities – World Cancer Research Fund, the American Institute for Cancer Research and Wereld Kanker Onderzoek Fonds – have funded 19 grants through our Regular Grant Programme (12 awards) and INSPIRE Research Challenge (7 awards), backing researchers who are pushing the boundaries of what’s possible in cancer prevention and cancer survivorship.
In total, £5,115,693.43 will be awarded from our network to projects led from 9 countries across the world. Of these 19 awards:
- 12 (63%) are focused on preventing cancer
- 7 (37%) are focused on helping people live better and longer after cancer
These grants range from global cohort studies using cutting-edge ‘omics’ technologies, to clinical trials testing exercise during chemotherapy, to innovative lifestyle interventions that survivors can use right now.
This year, their specific interests span everything from microplastics and air pollution, to insect-based fibre, ultra-processed foods in childhood, and exercise woven into cancer treatment.
Rethinking what’s on our plates (and in our environment)
Food, drink and environmental exposures are shaping cancer risk in ways science is only beginning to understand. Several of our new projects are tackling this head-on.
- Hidden DNA ‘typos’ in food and bowel cancer
At the University of Oxford, Professor Skirmantas Kriaucionis is investigating whether modified DNA building blocks can ‘sneak’ into our cells and damage our DNA, increasing the risk of bowel cancer. If certain cooking methods or ingredients generate these building blocks, this research could ultimately help people – and food producers – make safer choices. - Wholegrains vs refined grains across 20 cancers
At the Cancer Registry of Norway, Dr Dagfinn Aune is using data from more than 480,000 people to understand how whole grains and refined grains affect the risk of 20 different cancers. The findings will help show how many cancers might be prevented if more people swap refined grains for wholegrain options. - Sugar, soft drinks and pancreatic cancer
At the University of Padova, Dr Alessandro Carrer is exploring how fructose from sugary drinks may fuel early pancreatic cancer development. By pinpointing this pathway, the team hopes to clarify whether cutting back on certain sugary drinks could lower risk and inform future prevention strategies. - Ultra-processed foods in childhood and lifetime cancer risk
At Murdoch Children’s Research Institute, Dr Sherly (Xueyi) Li is leading the first comprehensive study to estimate how much ultra-processed food children are eating in Australia and 25 European countries, and how this might impact their future cancer risk. This project aims to provide crucial evidence for dietary guidelines and policies aimed at protecting children from unhealthy food environments. - Microplastics, air pollution and colorectal cancer
At IFOM in Milan, Dr Vito Amodio is asking whether microplastics, nanoplastics and tiny air pollution particles (like PM2.5) contribute to colorectal cancer by driving inflammation and disrupting the immune system. The results could inform both environmental policy and personal risk reduction. - Reducing colorectal cancer risk with cricket powder and chitin
At the University of Almeria, Dr Carmen Rodriguez Garcia is exploring whether chitin, a dietary fibre found in cricket powder, can help protect the bowel. By analysing samples from a completed dietary trial, the team will see how chitin affects gut bacteria, inflammation and chemical tags on DNA in the colon – all early warning signs for colorectal cancer. This innovative project links sustainable diets with cancer prevention and could inform future trials and dietary guidance.
Protecting people where the burden is highest
Cancer prevention isn’t just a high-income country issue. Several of our new awards are designed to address urgent evidence gaps in regions where the burden is particularly severe.
- Mycotoxins, infections and Burkitt lymphoma in African children
At IARC, Dr Rita Khoueiry is investigating how mycotoxins – toxic substances produced by moulds in staple foods – and Epstein-Barr virus combine to cause Burkitt lymphoma, a fast-growing childhood cancer in sub-Saharan Africa. By following a mother-child cohort from pregnancy and analysing biological samples over time, this work aims to identify modifiable risk factors and lay the groundwork for prevention strategies that protect children now and in future generations. - Oesophageal cancer precursors in the African Oesophageal Cancer Corridor
At IARC, Dr Valerie McCormack is leading a community-based study in Malawi to understand how dietary N-nitrosamines – carcinogens found in some traditional foods and drinks – and other lifestyle factors contribute to early changes in the oesophagus that can precede cancer. By identifying high-risk exposures, this work can inform local prevention strategies in one of the world’s highest-risk regions.
These projects are about levelling the playing field so that advances in cancer prevention benefit people everywhere – not just those living in wealthier countries.
Turning treatment time into healing time
Six of our new awards are focused on cancer survivorship – helping people with cancer live longer, better lives by embedding lifestyle support into care.
- Exercise during chemotherapy infusion for metastatic colon cancer
At the University of Sydney, Dr Kate Edwards is testing a simple but powerful idea: what if patients cycle on a stationary bike during their chemotherapy infusion, instead of sitting still. The EXERTION-mC trial will test whether this approach can improve tumour response, side effects and quality of life for people with metastatic colorectal cancer. - Exercise during immunotherapy for melanoma
At Australian Catholic University, Dr Eva Zopf is investigating whether a structured exercise programme is safe and feasible during adjuvant immunotherapy for people with melanoma – and whether it can improve side effects, wellbeing and immune responses. With immunotherapy now used widely for many cancers, this work could help shape future exercise-oncology recommendations. - Long-term benefits of exercise in metastatic breast cancer
At UMC Utrecht, Professor Anne May is following up participants from the large PREFERABLE-EFFECT trial to see whether the benefits of a 9-month supervised exercise programme – such as less fatigue and better quality of life – can be sustained 2–3 years later. Understanding long-term impact and cost-effectiveness is vital for integrating exercise as part of standard care for metastatic breast cancer. - Better sleep and support for people with primary brain tumours
At the University of Sydney, Dr Megan Jeon is testing telehealth group cognitive behavioural therapy for insomnia (CBT-I) for people living with primary brain tumours. Sleep problems are common and debilitating in this group yet often go untreated. This feasibility study will explore whether CBT-I, which is the gold standard nonpharmacological treatment, can safely improve sleep, mood and daily functioning in a population that has been largely overlooked in survivorship research. - Integrated lifestyle programme for cancer survivors
At the University of Colorado, Dr Emily Hill is developing and testing an integrated nutrition and exercise programme for post-treatment survivors that also includes sleep education, stress management and wearable technology such as smart watches and connected scales. By tracking stress, immune markers and behaviour change together, the study aims to show how lifestyle interventions improve health – and how to design programmes that survivors value and actually use. - Dietary fats and response to lung cancer immunotherapy
At the University of Torino, Professor Chiara Riganti will map “good” and “bad” fats in non-small cell lung cancer tumours to see which lipid patterns predict response to immunotherapy. The team will then test whether diets rich in “good” (mono- and poly-unsaturated) fats can boost treatment effectiveness in advanced laboratory models – enhancing immunotherapy and exploring other potential health benefits. - Balancing protein and fibre to support bowel cancer treatment
At Wageningen University, Dr Dieuwertje Kok is studying how the balance of protein and fibre in the diet affects recovery and long-term outcomes for people with bowel cancer. Using data from over 2,100 participants in the COLON study, plus a new dietary intervention, the team will examine how different combinations of protein and fibre relate to treatment complications, cancer recurrence and blood markers. The findings will help shape practical nutrition programmes to support patients through treatment and beyond.
Cracking the biology that links lifestyle to cancer
Several grants are focused on understanding how lifestyle factors ‘get under the skin’ to influence cancer risk, progression and response to treatment.
- Thyroid hormones, lifestyle and liver cancer risk
At IARC, Dr Mazda Jenab will investigate how thyroid hormone metabolism and lifestyle combine to influence liver cancer risk, using large international cohorts and genetic data. - Metabolic health, blood proteins and lifestyle-related cancers
At IARC, Dr Komodo Matta will use proteomics (large-scale protein profiling) to understand how metabolic health drives a range of lifestyle-related cancers – and identify blood protein signatures that could become targets for prevention. - Body composition, inflammation and multiple myeloma
At the University of Bristol, Dr Lucy Goudswaard will explore how body fat distribution and inflammation influence the development of multiple myeloma from its precursor condition, MGUS, helping to identify high-risk individuals and new intervention targets. - Exploring selenium and lung cancer risk
At the University of Southern Denmark, Professor Paolo Ceppi is investigating how selenium, a dietary mineral found in foods like nuts, meat and grains, influences the development of non-small cell lung cancer. By combining advanced lab studies with analysis of long-term selenium intake human populations, the goal is to provide clear, evidence-based guidance on selenium intake that could help reduce the burden of this deadly disease.
Together, these projects will help turn broad advice like “improve metabolic health” into precise pathways and actionable strategies.
Why this matters – and how donors make it possible
All of this science has one simple goal: fewer people getting cancer, and better lives for those who do.
From children growing up surrounded by ultra-processed foods and environmental pollutants, to adults at high risk of bowel, liver, pancreatic or oesophageal cancer, to people navigating life with metastatic breast cancer, brain tumours, melanoma or myeloma
These 19 projects are designed to produce the kind of robust, practical evidence that changes guidelines, shapes policy and transforms care.
None of it would be possible without the generosity of people and organisations who choose to support our work. Every donation – whether it’s a monthly gift, a legacy in a Will, or a fundraising challenge – helps us award more of this high-impact, prevention and survivorship-focused research. Thank you for supporting us.

Be the first to know
Want to be kept fully up-to-date with our research findings? Or learn more about our work helping people living with cancer?
Full list of research grants
Regular Grant Programme
1. Professor Anne May, University Medical Centre (UMC) Utrecht (UCMU), the Netherlands: Long-term effects of exercise on quality of life in patients with metastatic breast cancer: a follow-up study of the randomized PREFERABLE-EFFECT study – £224,213.65
2. Professor Paolo Ceppi, University of Southern Denmark, Denmark: Exploring Selenium and Lung Cancer Risk – £384,944.00
3. Dr Dagfinn Aune, Cancer Registry of Norway, Norway: Whole grains and refined grains and cancer incidence: habitual intakes, changes in intakes, substitutions and risk of 20 cancers in four Scandinavian cohort studies and a large American multiethnic cohort – £500,000.00
4. Dr Dieuwertje Kok Wageningen University, the Netherlands: Balancing dietary protein and fibre intake to improve outcomes of colorectal cancer treatment £464,411.00
5. Dr Rita Khoueiry, International Agency for Research on Cancer (IARC), France: Studying the impact of in-utero and early life exposure to mycotoxins on viral infections and the epigenome: unveiling the risk factors of endemic Burkitt Lymphoma in African children – £498,285.25
6. Dr Valerie McCormack, International Agency for Research on Cancer (IARC), France: Diet, N-nitrosamines and Esophageal Squamous Cell Carcinoma precursors in the African Esophageal Cancer Corridor: EndoSCCAPE – A community-based cross-sectional study in Malawi – £413,400.00
7. Professor Skirmantas Kriaucionis, University of Oxford, United Kingdom: Modified Nucleic Acids in Diet and Bowel Cancer Risk – £489,531.32
8. Dr Mazda Jenab, International Agency for Research on Cancer (IARC), France: Investigating the Role of Thyroid Hormone Metabolism in Liver Cancer Development: Integrating Lifestyle and Omics Data from Large Cohort Studies (HepaThyroid-omics) – £498,196.61
9. Dr Kate Edwards, University of Sydney, Australia: EXERTION-mC: EXERcise during chemoTherapy infusION to improve outcomes for people with metastatic Colon cancer – £499,242.00
10. Dr Alessandro Carrer, University of Padova, Italy: Interrogating the impact of fructose-to-acetate conversion for nucleolus organization and pancreatic cancer predisposition – £500,000.00
11. Dr Eva Zopf, Australian Catholic University, Australia: Safety and feasibility of exercise in patients with melanoma undergoing adjuvant immunotherapy with immune checkpoint inhibitor therapy – £59,519.00
12. Professor Chiara Riganti, University of Torino, Italy: Polyunsaturated fatty acids improve immunotherapy efficacy in non-small cell lung cancer – £60,000.00
Inspire Research Challenge
13. Dr Carmen Rodriguez, Garcia University of Almeria, Spain: Reducing Colorectal Cancer Risk with Cricket Powder and Chitin: Analysis of Epigenetic and Inflammatory Biomarkers from a Randomized Controlled Trial – £75,000.00
14. Dr Lucy Goudswaard, University of Bristol, United Kingdom: Characterising the role of body composition and inflammation in multiple myeloma – £74,950.60
15. Dr Komodo Matta, International Agency for Research on Cancer (IARC), France: Understanding the role of metabolic health in lifestyle related cancers through proteomics – £74,100.00
16. Dr Sherly (Xueyi) Li, Murdoch Children’s Research Institute, Australia: Ultra-processed food intake in childhood and their link to future risk of cancer – £75,000.00
17. Dr Vito Amodio, IFOM ETS – The AIRC institute of Molecular Oncology, Italy: Dissecting the impact of exposure to environmental pollutants on chronic inflammation and colorectal cancer onset – £74,900.00
18. Dr Megan Jeon, University of Sydney, Australia: A phase II single-arm feasibility study of telehealth group cognitive behavioural therapy for insomnia (CBT-I) in adults with primary brain tumours using a novel online platform for a stepped clinical pathway for sleep disturbance – £75,000.00
19. Dr Emily Hill, Regents of the University of Colorado, United States: Impact of an integrated nutrition and exercise program for post-treatment survivors on sleep quality, perceived stress, and biomarkers of immune dysregulation – £75,000.00
Latest news and blogs
At World Cancer Research Fund, we’re proud to launch Cook through cancer: Meals that matter, a new cookbook designed to support people living with and beyond cancer. The recipes were developed by Gopi Chandratheva, a Registered Nutritionist who specialises in creating nourishing and delicious recipes for a range of health-focused organisations.
In this blog, Gopi shares her inspiration for the cookbook and how she approached developing recipes for people affected by cancer.
Creating recipes with purpose
We asked Gopi to share what went into developing the recipes for the new Cook through cancer cookbook.
“When developing recipes, I usually start with a brief. For example, with World Cancer Research Fund, I had to make sure they are in line with their Recommendations and previous recipes, that they are budget-friendly, nutritious and easily accessible to people. It’s also important to make sure everyone can follow along, so I time every step out.
“I’ll start by brainstorming a few ideas for what I can create, and then discuss which ones they’re interested in. One key consideration today is ensuring that the ingredients are affordable, given how expensive groceries have become. I also want to keep the method simple, avoiding any complicated techniques. From start to finish, each recipe usually takes me a few days to develop.
“Working with World Cancer Research Fund was wonderful. I tried to be mindful of the challenges people going through cancer treatment can experience, especially with regards to changes in their sense of taste or possible feelings of nausea.
“With all the myths out there about cancer, I’m so glad to be able to use my skills to help people using real, evidence-based information that can help make tasty, nutritious meals.”
Cooking classes that make a difference
Gopi also delivers some of our Cook Through Cancer classes, free online cookery sessions for people living with and beyond cancer. These classes combine practical cooking demonstrations with expert nutrition support.
Gopi says, “The classes are really enjoyable. I was a bit nervous because it’s been a while since I’ve done live cooking sessions, but it was really fun and lively.”
Each class includes an Oncology Specialist Dietitian who answers participants’ questions with evidence-based advice. Gopi is pleased that the classes have been a success:
“The participants have really enjoyed it, and they always go away smiling – that’s the most important thing for me.”
Gopi’s favourite recipe
Gopi has a favourite recipe from the cookbook and the classes she delivers:
 “My favourite recipe I’ve made for the classes is the Buddha bowl. It’s a go-to for me because it’s a balanced meal on its own but it’s so customisable.
“My favourite recipe I’ve made for the classes is the Buddha bowl. It’s a go-to for me because it’s a balanced meal on its own but it’s so customisable.
“You can add whatever leftovers you have, as long as they fill the different categories of vegetables, protein, complex carbs and healthy fats, you have a complete meal with all the necessary food groups. Plus, it’s quick!”
Top tips for cooking during cancer treatment
Gopi shared her top tips for cooking during cancer treatment:
- Try to think about meal prepping. Stocking your pantry with tinned pulses means you have a great source of iron and protein right on hand to add to stews and soups.
- Stock up your freezer – it’s a great resource for keeping frozen fruit and veg and other ingredients that can help you make a meal in minutes.
- Batch cook and freeze your leftovers for an easy meal when you don’t feel up to cooking from scratch.
- Even something as simple as a slice of wholemeal toast with scrambled egg and spinach can make all the difference.
Get your copy
Whether you’re living with cancer, supporting someone who is or simply looking for nourishing recipes that are easy to prepare, Cook through cancer: Meals that matter is here to help.
Download your free copy or order a printed version today and start cooking meals that truly make a difference.
More about Gopi
When she isn’t devising tasty recipes, Gopi shares advice and information on healthy eating on Instagram. She also specialises in obesity and weight management providing one to ones, talks on nutrition, mentoring nutritionists and working for the NHS.
Gopi has been working in the nutrition field for many years with extensive experience and knowledge. She started working as a dietetic assistant in hospitals such as the Royal Marsden, where she developed her passion for helping those living with and beyond cancer.
Brought up in a family where food was central, Gopi has always been interested in food and health, and works hard to develop recipes that are as simple and delicious as they are good for you.
Find out more about Gopi: Her website | Follow her on Instagram


