This could help many people stay healthy, as there are 3 million vegetarians in the UK and interest is growing in many parts of the world.
The research, led by scientists at Oxford Population Health’s Cancer Epidemiology Unit, pooled data from more than 1.8 million people across three continents through the Cancer Risk in Vegetarians Consortium – the largest ever study of non-meat diets and cancer risk.
They compared the risk of 17 different cancers across five diet groups: meat eaters, poultry eaters (do not eat red or processed meat), pescatarians (fish eaters), vegetarians (eat dairy and/or eggs), and vegans.
Compared with meat eaters, vegetarians had:
- 21% lower risk of pancreatic cancer
- 9% lower risk of breast cancer
- 12% lower risk of prostate cancer
- 28% lower risk of kidney cancer
- 31% lower risk of multiple myeloma.
However, vegetarians had:
- Nearly double the risk of squamous cell carcinoma of the oesophagus.
Tim Key
Dietary patterns that prioritise fruit, vegetables, and fibre-containing foods, and avoid processed meat, are recommended to reduce cancer risk. Our study helps to shed light on the benefits and risks associated with vegetarian diets.
Aurora Perez Cornago,
The higher risk of oesophageal squamous cell carcinoma in vegetarians and bowel cancer in vegans may relate to lower intakes of certain nutrients more abundant in animal foods. Additional research is needed to understand what is driving the differences in cancer risk found in our study
Dr Helen Croker
The results suggest non-meat diets are linked to lower risks for some cancers, though not all, highlighting important differences between cancer types and the role of different dietary patterns. To increase your overall protection from cancer, our advice is to build meals around wholegrains, pulses, fruit and vegetables, and avoid processed meat and limit red meat.
Yashvee Dunneram
Among the 72,000 vegetarians and vegans included in our study, the numbers of cases for some cancers were small, which limits the certainty of some findings. Moreover, nutrient intakes and overall diet quality vary substantially within and between vegetarian populations. Our next challenge is to collect more data on vegan diets and more data from other parts of the world.
There were no statistically-significant differences in risk for colorectal, stomach, liver, lung (in never smokers), endometrial, ovarian, mouth and pharynx, or bladder cancers, or non-Hodgkin lymphoma, leukaemia, and oesophageal adenocarcinoma in vegetarians.
Vegans had a statistically significant higher risk of colorectal (bowel) cancer when compared with meat eaters. For the other cancers studied, there was no evidence that risk in vegans differed from meat eaters, and for some less common cancers there were too few vegan cases to analyse. Further studies are needed to confirm these results in the vegan population.
Pescatarians had lower risks of breast and kidney cancers, as well as a lower risk of bowel cancer. Poultry eaters were found to have a lower risk of prostate cancer.
The full findings were published on 27 February 2026 in the British Journal of Cancer.
Latest news and blogs



World Cancer Research Fund’s Executive Director of Research and Policy, Dr Giota Mitrou, said: “On International Childhood Cancer Day, it is heartening to see global attention focused on the children and young people, and their loved ones, whose lives are changed by cancer.
We are proud to support studies that help us better understand how nutrition, physical activity and other lifestyle factors influence both risk and survivorship, and to ensure that childhood cancer remains firmly on the health agenda.
Each year, over 400,000 children and adolescents are diagnosed with cancer.
The rate of survival depends on the region. Children and young people with cancer have an 80% chance of survival in most High-Income Countries, but this drops to as low as 20% in Low- and Middle-Income Countries.
International Childhood Cancer Day is held on the 15 February each year. Childhood cancer affects individuals and families all year round, but the day itself provides a moment for us to raise awareness and develop a deeper understanding of the unique issues and challenges faced by those whose lives are touched by childhood cancer.
It also spotlights the need for more equitable and better access to treatment and care for all children with cancer, everywhere.
The World Health Organization (WHO) Global Childhood Cancer Initiative has a goal of increasing the survival rate of children with cancer to at least 60% by 2030, while reducing the suffering and improving the quality of life for all children living with cancer.
This goal can be achieved by increasing capacity to provide quality services for children with cancer around the world, and by prioritising childhood cancer at global, regional and national levels.
The recently-published National Cancer Plan for England places renewed emphasis on improving the nutritional care of children and young people undergoing cancer treatment, recognising that good nutrition is fundamental to treatment tolerance, recovery, and long‑term survival.
This focus on nutrition highlights the wider need for sustained research into childhood cancer that will strengthen our knowledge of how early‑life exposures, diet, physical activity, and environment shape both risk and survivorship.
Across the World Cancer Research Fund (WCRF) network of charities, we are funding studies that explore these factors and their impact on the lives of children and young people affected by cancer.
Using AI chatbots to support families of children with cancer
Dr Micah Skeens was funded by World Cancer Research Fund to test an AI powered chatbot called DAPHNE, designed to identify and manage the social and emotional needs of families caring for a child with cancer.
The research team found that the tool had high usability, and positive feedback from caregivers suggest that it can be an important resource is supporting families. By integrating AI technology into cancer care, it has the potential to revolutionise the identification and management of social needs in paediatric oncology.
Studying Burkitt lymphoma among children in sub-Saharan Africa
Dr Rita Khoueiry is funded by Wereld Kanker Onderzoek Fonds (WKOF) – our network charity in the Netherlands – to understand whether exposure to mycotoxins and infection with Epstein-Barr virus put children at risk of Burkitt lymphoma.
The research is exploring how in-utero and early-life exposure to mycotoxins (toxic compounds produced by fungi) may contribute, in combination with viruses and parasites, to the development of diseases such as Burkitt lymphoma, the most common childhood cancer in sub-Saharan Africa.
Understanding this relationship will set the foundation for developing new prevention strategies to protect at risk children.
Since food contamination with mycotoxins is expected to increase due to climate change, the results are of growing interest worldwide.
The FITco study: Can nutrition and exercise give children with cancer a better chance of survival?
Professor Wim Tissing and Dr Dieuwertje Kok are leading on FITco – a unique long-term study looking at body composition, nutritional intake and exercise in children with cancer.
The FITco study, launched in May 2025, is run by the Princess Máxima Center and Wageningen University & Research, and funded by WKOF.
FITco will follow 500 children newly diagnosed with cancer, tracking their diet, physical activity, and body composition. By understanding how these factors influence treatment, side‑effects, and long‑term health, the team aims to identify better ways to support children during and after cancer therapy.
With strong international collaborations, this research has the potential to shape global standards of supportive care in paediatric oncology.
Real-time tracking of environments and well‑being in young adults with cancer
Dr Katie Darabos is being funded by the American Institute for Cancer Research (AICR) to assess how aspects of the lived environment, and the movement of young adult cancer survivors, influences health behaviours.
Using GPS technology and real‑time surveys, Dr Darabos and team hope to understand how the environments young adults move through each day influence their stress levels, health behaviours, and overall well‑being.
By identifying the types of neighbourhoods or daily settings that increase stress or make healthy choices harder, this research will help pinpoint potential high‑risk environments.
The long‑term impact is significant – it could enable the development of targeted, mobile‑based interventions that support young cancer survivors exactly when and where they need it most.
Smart scans, stronger futures: AI and body composition in paediatric cancer survivorship
Funded by AICR, Dr Paul Yi is developing an AI‑powered tool to analyse routine CT scans and uncover how changes in body composition, such as muscle and fat levels, relate to treatment outcomes in children with cancer.
Right now, it is challenging to predict which survivors of childhood cancer will face serious health impacts down the line.
By revealing patterns that clinicians may not otherwise detect, the insights from this work could transform ongoing survivorship care. This research has the potential to help cancer survivors achieve better long-term health, reduce serious complications that often arise years later, and improve their quality of life.
Diet and exercise to improve treatment outcomes in B‑cell acute lymphoblastic leukaemia
Obesity contributes to the risk for developing acute lymphoblastic leukaemia. It is also known to increase the chance of chemotherapy being less effective and the disease returning in those being treated for it.
Dr Etan Orgel is testing whether targeted diet and physical activity interventions can reduce obesity risk during treatment for B‑cell acute lymphoblastic leukaemia.
This study, funded by AICR, has the potential to identify practical, evidence‑based strategies that make chemotherapy more effective and improve survival outcomes for children and adolescents living with this common childhood cancer.
Digital technologies to understand and improve physical activity in adolescents and young adults
Dr Lisa Schwartz is using innovative tools, including wearable activity monitors and real‑time surveys, to understand the daily factors that influence physical activity in adolescents and young adults with cancer.
By capturing the barriers that prevent young people from being active, this AICR funded research could pave the way for personalised interventions that help them overcome these challenges.
Ultimately, the aim of this research is to assist adolescents and young adults undergoing cancer treatment to be more physically active, which may ease their treatment symptoms and improve their mood and quality of life.
It has long been established that junk food advertising drives consumption of unhealthy food and drink, shaping preferences from a young age and contributing to overweight and obesity.
The strength of the evidence base is perhaps best corroborated by the enormous advertising budgets of unhealthy food and drink companies. If advertising didn’t pay off, why would Coca-Cola allocate a whopping $5 billion to their worldwide advertising budget in 2024?
Restricting junk food advertising is therefore a powerful and proven public health measure. Yet, most recently, you may have seen measured responses from public health advocates in the UK, including World Cancer Research Fund, upon the introduction of long-awaited junk food advertising restrictions in January 2026.
Marketing regulations can underdeliver
The bottom line is that whilst the UK’s restrictions mark a step forward in protecting children’s health at a time when obesity rates continue to rise, they have been weakened and delayed by industry influence – most notably through the introduction of a sweeping brand exemption. This significantly undermines the policy in two key ways. First, it allows brands that are synonymous with foods high in fat, salt and sugar (HFSS) to continue being advertised – think the famous Golden Arches. Second, the lack of brand restrictions enables companies to promote entire HFSS product ranges, just not individual products. Ultimately this preserves brand visibility and influence while circumventing the spirit of the regulations.
The brand exemption is not the only weakness of the advertising restrictions. Work on this policy began as far back as 2018, and in the years since, the marketing landscape has evolved dramatically. Simply put, the regulations are not a match for the rapidly changing marketing landscape. For example, direct marketing channels, such as email and text messaging, remain unchecked, allowing unhealthy food and drink companies to continue targeting consumers.
The unseen cost of delays and dilution
The unfortunate tale of industry influence is not unique to the UK. Globally, efforts to curb the scourge of junk food on society are denied, diluted, derailed and delayed by industry.
Marketing restrictions are difficult to get over the line. In the UK, the policy was subject to five separate consultations and four delays to its rollout. That is an immense amount of government time, effort and resources. Moreover, the burden it places on the public health sector, which often operate under capacity constraints, must be acknowledged.
We also need to recognise that obesity, a key risk factor for cancer, is linked to deprivation. In many countries, those living in the most deprived areas are more likely to be living with obesity compared to those in the most affluent communities. Delays or failures to implement effective policies therefore disproportionately impact those who are already most vulnerable.
Industry opposition at full throttle
The resistance we see to advertising restrictions can partly be explained by the fact that marketing is not a peripheral commercial function. Instead, it sits at the very core of food and drink businesses, playing a pivotal role in building brand value, customer loyalty and long-term profitability.
Marketing restrictions are also unusually visible. Unlike reformulation targets or nutrient thresholds, which operate largely behind the scenes, advertising bans are immediately noticeable. They can also be drawn into wider debates around personal responsibility, censorship and creativity – making the more contested and politically charged. They tend to hit a nerve.
Recognition of these issues is not a justification for inaction. The reality is that companies by their very nature are required to innovate, and they can do so in a way that supports public health rather than undermining it.
Action must go beyond the status quo
Let’s be clear, no one is suggesting that junk food marketing restrictions alone will solve the obesity crisis. However, the version we’ve seen introduced in the UK will most certainly underdeliver, especially given the restrictions don’t sit within a broader framework of measures designed to improve the nation’s diet yet. Countries in Latin America, including Chile and Mexico, have taken more holistic approaches which embed marketing restrictions within a wider set of measures including mandatory warning labels and robust school food standards
But when governments introduce policies that appear ambitious on paper but lack the strength to deliver in practice, they risk entrenching the status quo while giving the impression of action. This pattern is not unique to food. Similar delays and dilutions are seen across alcohol, gambling and other health-harming industries, where commercial interests routinely take priority over public health.
Ultimately, the question is not what needs to be done, but what governments are willing to do to protect public health.
Related news and blogs


World Cancer Research Fund – part of the World Cancer Research Fund network – welcomes many of the recommendations in the new US Dietary Guidelines for Americans that support healthier diets and reduce the burden of diet-related disease.
When it comes to cancer prevention, we have some concerns with the guidelines relating to alcohol and red and processed meat.
The strong emphasis on healthy dietary patterns, including increased consumption of fruits, vegetables and wholegrains, is very helpful – as are the recommendations to limit highly processed foods and products high in added sugars. The clear inclusion of plant-source protein foods – such as beans, lentils, nuts, seeds and soy – is also positive.
The guidance to drink mainly water and to avoid sugar-sweetened beverages and consume less alcohol is helpful, as we know there is no safe level of drinking alcohol when it comes to cancer prevention. Finally, we strongly welcome support for breastfeeding.
These Guidelines help to translate evidence into clear public advice and shape future policies. However, from a cancer prevention perspective, the Guidelines’ increased emphasis on animal-source proteins, and particularly the emphasis on red meat, is at odds with the scientific evidence linking higher intakes of red and processed meat to increased cancer risk.
Similarly, the promotion of whole-fat dairy raises concerns, given the potential contribution to excess weight gain. In light of such issues, we remain committed to informing the public with authoritative advice, which we develop based on the latest scientific evidence from leading researchers worldwide.
Below is a more detailed summary of the what the Guidelines mean for cancer prevention.
Important takeaways from the guidance
- Clear guidance is provided to prioritise whole foods and limit highly processed products, including advice to avoid salty and sweet packaged snacks and to favour nutrient-dense, home-prepared meals. This approach is closely aligned with our emphasis on limiting fast foods and processed foods high in fat, starches and sugars, and on reducing overall dietary energy density as a pathway to achieving a healthier body weight and lowering cancer risk.
- The Guidelines strengthen the stance on added sugars and sugar-sweetened beverages, including explicit recommendations to limit consumption of sugar-sweetened drinks and to limit added sugars at meals. This aligns well with our evidence of sugar intake as a contributor to excess weight gain and poorer overall diet quality.
- Plant foods remain important to the guidance, with daily targets for fruit and vegetable intake and a clear recommendation to prioritise fibre-rich whole grains. This maps directly onto our emphasis on dietary and lifestyle patterns and core cancer prevention recommendations.
- Breastfeeding is explicitly encouraged, with guidance to breastfeed exclusively for the first six months and to continue breastfeeding for two years or beyond. This is consistent with our recommendation that mothers breastfeed where possible and complements the focus on breast cancer prevention.
Important clarifications based on our global scientific research
- The Guidelines place a strong emphasis on increasing protein intake, explicitly including red meat and setting a higher quantitative protein target.
From a cancer prevention perspective, this emphasis would benefit from clearer direction to prioritise plant-based protein sources such as tofu, beans, lentils and other legumes, as well as nuts, seeds, fish and poultry, while reiterating World Cancer Research Fund guidance to limit red meat consumption and avoid processed meat altogether. - Furthermore, the Guidelines promote protein-rich foods, in relation to meat; specifically, meat with no or limited added sugars, refined starches or chemical additives is recommended. Avoidance of processed meat aligns with our recommendation to eat little, if any, processed meat based on strong evidence of an increased risk of colorectal cancer.
- While the Guidelines prioritise fibre-rich wholegrains, they do not have significant prominence in the new ‘Real Food’ pyramid, which undermines their importance.
- The Guidelines adopt a general recommendation to consume less alcohol. For cancer prevention, it is best not to drink alcohol at all, as there is no safe threshold of consumption for cancer risk for at least seven cancer types.
- The explicit endorsement of full-fat dairy, with guidance to consume three servings per day, warrants careful interpretation given its contribution to excess weight and some variation in evidence by cancer site. Framing dairy as one possible option, rather than a central or universal recommendation, may therefore be more appropriate.
- The Guidelines’ discussion of “healthy fats” includes foods such as butter and beef tallow, while still recommending that saturated fat remain below 10% of total energy intake.
This recommendation needs careful explanation because butter and beef tallow are high in saturated fat and can affect overall energy balance. Maintenance of a healthy weight is important, as overweight and obesity increase the risk of at least 13 cancers.
Three important policy implications for the future
- Affordability and access: Achieving the dietary pattern outlined in the guidelines will require targeted policy measures to improve the availability and affordability of fresh and whole foods. At present, such diets remain out of reach for many Americans, particularly those on lower incomes. Without significant structural interventions there is a risk that the guidelines may exacerbate existing health inequalities.
- Clarity and implementation: Greater clarity is needed on how “highly processed foods” are defined within the guidelines and how this definition will be operationalised. Clear definitions are essential to inform coherent policy action, regulation, monitoring and public communication.
- Policy alignment and delivery: It remains unclear whether new or strengthened policy measures will be introduced to support the recommended dietary changes, or how these guidelines will be embedded across food, agriculture, procurement and public health policies to enable meaningful implementation. In addition, the guidelines should also consider broader factors such as sustainability and planetary health.
Explore our research
More useful information
Understanding the origins of bowel cancer risk
Our funded research showed greater birthweight or body size during childhood, adolescence or young adulthood was linked with higher risk of bowel cancer in later life.
It was the first CUP Global review to analyse and judge all the research examining how factors such as weight, height and body size in early life relate to our risk of bowel cancer as we get older.
Brisk walking cold reduce your cancer risk
Our funded researchers published evidence that brisk walking is linked to a lower risk of 5 cancers, including anal, liver, small intestine, thyroid, and lung.
Smaller waist or more exercise? For cancer prevention, both is best
In the world’s first study looking at the effectiveness of combining maintaining a smaller waist with staying active, we found that only doing one is not enough to lower our risk of cancer.
The study found that people not meeting World Health Organization (WHO) guidelines on waist circumference are at 11% greater risk, even if they are physically active.
And people not meeting WHO guidelines for physical exercise are at 4% greater risk, even if “abdominally lean” (i.e. they have a smaller waist). Achieving neither means a 15% greater risk.
The simple rule that cuts cancer risk by 23%
We released a first-of-its-kind study into how the number of different food types consumed, measured as Dietary Species Richness (the number of species an individual consumes per year) affects the risk of developing gastrointestinal cancer.
The study found that individuals with the most diverse diets had a 23% lower risk of developing gastrointestinal cancers compared with those with the least variety. The risk decreased by 6% for every 10 extra species per year added to their diet.
The growing need for your support
Your generous donations have enabled us to fund 19 new research grants this year, worth a total of £5 million, bringing our network’s achievements over the last 20 years to more than 200 research grants awarded and over £50m invested in research overall.
Over the past year, 13 projects came to a close, delivering inspiring new findings. These completed studies explored many ways to prevent cancer, improve treatment, and support people living with and beyond the disease. They examined how factors like body weight, nutrition, inflammation, and even sleep patterns may influence cancer risk, treatment side effects, and recovery.
Some looked at how early-life infections, obesity, and physical activity can affect cancer risk later in life, while others tested promising treatments or searched for new ways to use cancer drugs. There were also studies researching how to help people living with and beyond cancer live healthier lives, from technology-based tools and personalised vitamin D supplements to culturally tailored support for Indigenous communities and families of children with cancer.
As the number of cancer diagnoses grows worldwide, research into cancer prevention is more vital than ever. Thanks to your continuing support, we can continue to fund novel and innovative research and push the boundaries of knowledge on cancer research so that fewer people die from a preventable cancer.

Donations from our fantastic supporters are smartly invested into the most impactful opportunities in science, guided by our wide network of independent leading experts.
Each year, millions of people hear the words “you have cancer” – and millions more are quietly edging towards a preventable diagnosis because of factors like diet, weight, inactivity or environmental exposures.
There’s a huge opportunity here: we know that 40% of cancer cases could be prevented. But there are still major gaps in the evidence that our latest round of awards will help to fill.
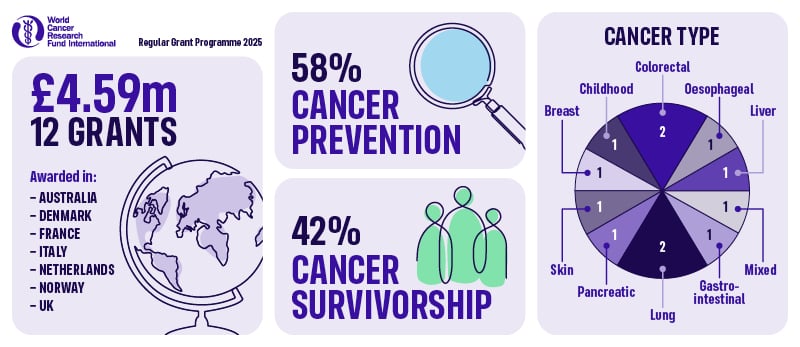
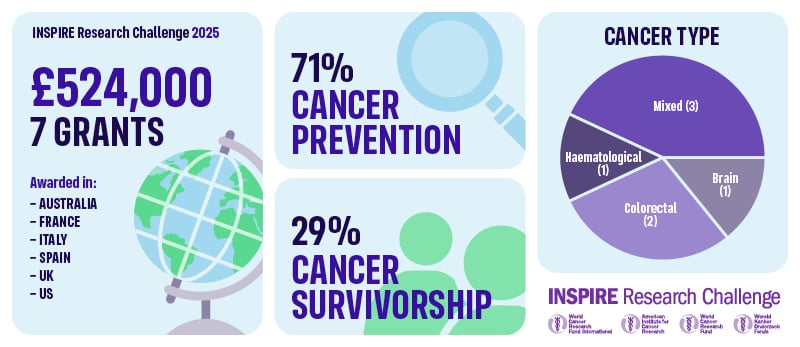
The three charities – World Cancer Research Fund, the American Institute for Cancer Research and Wereld Kanker Onderzoek Fonds – have funded 19 grants through our Regular Grant Programme (12 awards) and INSPIRE Research Challenge (7 awards), backing researchers who are pushing the boundaries of what’s possible in cancer prevention and cancer survivorship.
In total, £5,115,693.43 will be awarded from our network to projects led from 9 countries across the world. Of these 19 awards:
- 12 (63%) are focused on preventing cancer
- 7 (37%) are focused on helping people live better and longer after cancer
These grants range from global cohort studies using cutting-edge ‘omics’ technologies, to clinical trials testing exercise during chemotherapy, to innovative lifestyle interventions that survivors can use right now.
This year, their specific interests span everything from microplastics and air pollution, to insect-based fibre, ultra-processed foods in childhood, and exercise woven into cancer treatment.
Rethinking what’s on our plates (and in our environment)
Food, drink and environmental exposures are shaping cancer risk in ways science is only beginning to understand. Several of our new projects are tackling this head-on.
- Hidden DNA ‘typos’ in food and bowel cancer
At the University of Oxford, Professor Skirmantas Kriaucionis is investigating whether modified DNA building blocks can ‘sneak’ into our cells and damage our DNA, increasing the risk of bowel cancer. If certain cooking methods or ingredients generate these building blocks, this research could ultimately help people – and food producers – make safer choices. - Wholegrains vs refined grains across 20 cancers
At the Cancer Registry of Norway, Dr Dagfinn Aune is using data from more than 480,000 people to understand how whole grains and refined grains affect the risk of 20 different cancers. The findings will help show how many cancers might be prevented if more people swap refined grains for wholegrain options. - Sugar, soft drinks and pancreatic cancer
At the University of Padova, Dr Alessandro Carrer is exploring how fructose from sugary drinks may fuel early pancreatic cancer development. By pinpointing this pathway, the team hopes to clarify whether cutting back on certain sugary drinks could lower risk and inform future prevention strategies. - Ultra-processed foods in childhood and lifetime cancer risk
At Murdoch Children’s Research Institute, Dr Sherly (Xueyi) Li is leading the first comprehensive study to estimate how much ultra-processed food children are eating in Australia and 25 European countries, and how this might impact their future cancer risk. This project aims to provide crucial evidence for dietary guidelines and policies aimed at protecting children from unhealthy food environments. - Microplastics, air pollution and colorectal cancer
At IFOM in Milan, Dr Vito Amodio is asking whether microplastics, nanoplastics and tiny air pollution particles (like PM2.5) contribute to colorectal cancer by driving inflammation and disrupting the immune system. The results could inform both environmental policy and personal risk reduction. - Reducing colorectal cancer risk with cricket powder and chitin
At the University of Almeria, Dr Carmen Rodriguez Garcia is exploring whether chitin, a dietary fibre found in cricket powder, can help protect the bowel. By analysing samples from a completed dietary trial, the team will see how chitin affects gut bacteria, inflammation and chemical tags on DNA in the colon – all early warning signs for colorectal cancer. This innovative project links sustainable diets with cancer prevention and could inform future trials and dietary guidance.
Protecting people where the burden is highest
Cancer prevention isn’t just a high-income country issue. Several of our new awards are designed to address urgent evidence gaps in regions where the burden is particularly severe.
- Mycotoxins, infections and Burkitt lymphoma in African children
At IARC, Dr Rita Khoueiry is investigating how mycotoxins – toxic substances produced by moulds in staple foods – and Epstein-Barr virus combine to cause Burkitt lymphoma, a fast-growing childhood cancer in sub-Saharan Africa. By following a mother-child cohort from pregnancy and analysing biological samples over time, this work aims to identify modifiable risk factors and lay the groundwork for prevention strategies that protect children now and in future generations. - Oesophageal cancer precursors in the African Oesophageal Cancer Corridor
At IARC, Dr Valerie McCormack is leading a community-based study in Malawi to understand how dietary N-nitrosamines – carcinogens found in some traditional foods and drinks – and other lifestyle factors contribute to early changes in the oesophagus that can precede cancer. By identifying high-risk exposures, this work can inform local prevention strategies in one of the world’s highest-risk regions.
These projects are about levelling the playing field so that advances in cancer prevention benefit people everywhere – not just those living in wealthier countries.
Turning treatment time into healing time
Six of our new awards are focused on cancer survivorship – helping people with cancer live longer, better lives by embedding lifestyle support into care.
- Exercise during chemotherapy infusion for metastatic colon cancer
At the University of Sydney, Dr Kate Edwards is testing a simple but powerful idea: what if patients cycle on a stationary bike during their chemotherapy infusion, instead of sitting still. The EXERTION-mC trial will test whether this approach can improve tumour response, side effects and quality of life for people with metastatic colorectal cancer. - Exercise during immunotherapy for melanoma
At Australian Catholic University, Dr Eva Zopf is investigating whether a structured exercise programme is safe and feasible during adjuvant immunotherapy for people with melanoma – and whether it can improve side effects, wellbeing and immune responses. With immunotherapy now used widely for many cancers, this work could help shape future exercise-oncology recommendations. - Long-term benefits of exercise in metastatic breast cancer
At UMC Utrecht, Professor Anne May is following up participants from the large PREFERABLE-EFFECT trial to see whether the benefits of a 9-month supervised exercise programme – such as less fatigue and better quality of life – can be sustained 2–3 years later. Understanding long-term impact and cost-effectiveness is vital for integrating exercise as part of standard care for metastatic breast cancer. - Better sleep and support for people with primary brain tumours
At the University of Sydney, Dr Megan Jeon is testing telehealth group cognitive behavioural therapy for insomnia (CBT-I) for people living with primary brain tumours. Sleep problems are common and debilitating in this group yet often go untreated. This feasibility study will explore whether CBT-I, which is the gold standard nonpharmacological treatment, can safely improve sleep, mood and daily functioning in a population that has been largely overlooked in survivorship research. - Integrated lifestyle programme for cancer survivors
At the University of Colorado, Dr Emily Hill is developing and testing an integrated nutrition and exercise programme for post-treatment survivors that also includes sleep education, stress management and wearable technology such as smart watches and connected scales. By tracking stress, immune markers and behaviour change together, the study aims to show how lifestyle interventions improve health – and how to design programmes that survivors value and actually use. - Dietary fats and response to lung cancer immunotherapy
At the University of Torino, Professor Chiara Riganti will map “good” and “bad” fats in non-small cell lung cancer tumours to see which lipid patterns predict response to immunotherapy. The team will then test whether diets rich in “good” (mono- and poly-unsaturated) fats can boost treatment effectiveness in advanced laboratory models – enhancing immunotherapy and exploring other potential health benefits. - Balancing protein and fibre to support bowel cancer treatment
At Wageningen University, Dr Dieuwertje Kok is studying how the balance of protein and fibre in the diet affects recovery and long-term outcomes for people with bowel cancer. Using data from over 2,100 participants in the COLON study, plus a new dietary intervention, the team will examine how different combinations of protein and fibre relate to treatment complications, cancer recurrence and blood markers. The findings will help shape practical nutrition programmes to support patients through treatment and beyond.
Cracking the biology that links lifestyle to cancer
Several grants are focused on understanding how lifestyle factors ‘get under the skin’ to influence cancer risk, progression and response to treatment.
- Thyroid hormones, lifestyle and liver cancer risk
At IARC, Dr Mazda Jenab will investigate how thyroid hormone metabolism and lifestyle combine to influence liver cancer risk, using large international cohorts and genetic data. - Metabolic health, blood proteins and lifestyle-related cancers
At IARC, Dr Komodo Matta will use proteomics (large-scale protein profiling) to understand how metabolic health drives a range of lifestyle-related cancers – and identify blood protein signatures that could become targets for prevention. - Body composition, inflammation and multiple myeloma
At the University of Bristol, Dr Lucy Goudswaard will explore how body fat distribution and inflammation influence the development of multiple myeloma from its precursor condition, MGUS, helping to identify high-risk individuals and new intervention targets. - Exploring selenium and lung cancer risk
At the University of Southern Denmark, Professor Paolo Ceppi is investigating how selenium, a dietary mineral found in foods like nuts, meat and grains, influences the development of non-small cell lung cancer. By combining advanced lab studies with analysis of long-term selenium intake human populations, the goal is to provide clear, evidence-based guidance on selenium intake that could help reduce the burden of this deadly disease.
Together, these projects will help turn broad advice like “improve metabolic health” into precise pathways and actionable strategies.
Why this matters – and how donors make it possible
All of this science has one simple goal: fewer people getting cancer, and better lives for those who do.
From children growing up surrounded by ultra-processed foods and environmental pollutants, to adults at high risk of bowel, liver, pancreatic or oesophageal cancer, to people navigating life with metastatic breast cancer, brain tumours, melanoma or myeloma
These 19 projects are designed to produce the kind of robust, practical evidence that changes guidelines, shapes policy and transforms care.
None of it would be possible without the generosity of people and organisations who choose to support our work. Every donation – whether it’s a monthly gift, a legacy in a Will, or a fundraising challenge – helps us award more of this high-impact, prevention and survivorship-focused research. Thank you for supporting us.

Be the first to know
Want to be kept fully up-to-date with our research findings? Or learn more about our work helping people living with cancer?
Full list of research grants
Regular Grant Programme
1. Professor Anne May, University Medical Centre (UMC) Utrecht (UCMU), the Netherlands: Long-term effects of exercise on quality of life in patients with metastatic breast cancer: a follow-up study of the randomized PREFERABLE-EFFECT study – £224,213.65
2. Professor Paolo Ceppi, University of Southern Denmark, Denmark: Exploring Selenium and Lung Cancer Risk – £384,944.00
3. Dr Dagfinn Aune, Cancer Registry of Norway, Norway: Whole grains and refined grains and cancer incidence: habitual intakes, changes in intakes, substitutions and risk of 20 cancers in four Scandinavian cohort studies and a large American multiethnic cohort – £500,000.00
4. Dr Dieuwertje Kok Wageningen University, the Netherlands: Balancing dietary protein and fibre intake to improve outcomes of colorectal cancer treatment £464,411.00
5. Dr Rita Khoueiry, International Agency for Research on Cancer (IARC), France: Studying the impact of in-utero and early life exposure to mycotoxins on viral infections and the epigenome: unveiling the risk factors of endemic Burkitt Lymphoma in African children – £498,285.25
6. Dr Valerie McCormack, International Agency for Research on Cancer (IARC), France: Diet, N-nitrosamines and Esophageal Squamous Cell Carcinoma precursors in the African Esophageal Cancer Corridor: EndoSCCAPE – A community-based cross-sectional study in Malawi – £413,400.00
7. Professor Skirmantas Kriaucionis, University of Oxford, United Kingdom: Modified Nucleic Acids in Diet and Bowel Cancer Risk – £489,531.32
8. Dr Mazda Jenab, International Agency for Research on Cancer (IARC), France: Investigating the Role of Thyroid Hormone Metabolism in Liver Cancer Development: Integrating Lifestyle and Omics Data from Large Cohort Studies (HepaThyroid-omics) – £498,196.61
9. Dr Kate Edwards, University of Sydney, Australia: EXERTION-mC: EXERcise during chemoTherapy infusION to improve outcomes for people with metastatic Colon cancer – £499,242.00
10. Dr Alessandro Carrer, University of Padova, Italy: Interrogating the impact of fructose-to-acetate conversion for nucleolus organization and pancreatic cancer predisposition – £500,000.00
11. Dr Eva Zopf, Australian Catholic University, Australia: Safety and feasibility of exercise in patients with melanoma undergoing adjuvant immunotherapy with immune checkpoint inhibitor therapy – £59,519.00
12. Professor Chiara Riganti, University of Torino, Italy: Polyunsaturated fatty acids improve immunotherapy efficacy in non-small cell lung cancer – £60,000.00
Inspire Research Challenge
13. Dr Carmen Rodriguez, Garcia University of Almeria, Spain: Reducing Colorectal Cancer Risk with Cricket Powder and Chitin: Analysis of Epigenetic and Inflammatory Biomarkers from a Randomized Controlled Trial – £75,000.00
14. Dr Lucy Goudswaard, University of Bristol, United Kingdom: Characterising the role of body composition and inflammation in multiple myeloma – £74,950.60
15. Dr Komodo Matta, International Agency for Research on Cancer (IARC), France: Understanding the role of metabolic health in lifestyle related cancers through proteomics – £74,100.00
16. Dr Sherly (Xueyi) Li, Murdoch Children’s Research Institute, Australia: Ultra-processed food intake in childhood and their link to future risk of cancer – £75,000.00
17. Dr Vito Amodio, IFOM ETS – The AIRC institute of Molecular Oncology, Italy: Dissecting the impact of exposure to environmental pollutants on chronic inflammation and colorectal cancer onset – £74,900.00
18. Dr Megan Jeon, University of Sydney, Australia: A phase II single-arm feasibility study of telehealth group cognitive behavioural therapy for insomnia (CBT-I) in adults with primary brain tumours using a novel online platform for a stepped clinical pathway for sleep disturbance – £75,000.00
19. Dr Emily Hill, Regents of the University of Colorado, United States: Impact of an integrated nutrition and exercise program for post-treatment survivors on sleep quality, perceived stress, and biomarkers of immune dysregulation – £75,000.00
Latest news and blogs
There aren’t many things in life you run straight into without testing first. Plays need rehearsals, restaurants need test kitchens, and researchers need feasibility studies.
Think about pilot and feasibility studies like the first walk-through of a play. You’re planning a large-scale production, and you want it to be a success – you can’t just go straight into the performance. First, you need to suss out: have you got the script right? Can you get the actors in the roles? Will the show be a hit?
It’s the same with feasibility studies. Before you run a big trial, with a lot of time, funding, and resources thrown into it, you need to figure out whether the whole thing is actually possible!
What do pilot and feasibility studies aim to achieve?
The aim of both pilot and feasibility studies, yes – you’ve guessed it – is to see if a study is feasible. A pilot study tests the exact design of a larger future trial; it’s essentially a mini version. A feasibility study differs in that it doesn’t have to follow the exact design of the planned trial, instead it can explore various aspects of the study’s design to find out what works best.
These studies are the prime time to ask key questions and put them to the test in real life. These include questions about:
- Recruitment and retention: can you realistically get enough people to take part in the trial? And not only will they sign up, but will they stay for the whole duration?
- Acceptability and adherence: are participants and staff happy with the study plan and assessments that are carried out? And do they follow it as planned?
- Data: is the data collected reliable, complete, and good quality?
- Resources: have you factored in all the relevant ingredients? Do you have enough time, staff and money to run it as planned?
- Method: is this study recipe one that can be followed smoothly?
- Safety: are there any safety concerns that could prevent scaling up?
Without testing, it can be hard to know. The science could be spot on, the study beautifully designed, but if participants don’t like it or professionals find delivering it a burden, then you don’t have a successful trial on your hands.
Therefore, researchers take this chance to identify and explore potential challenges before the main trial begins. By tackling these issues early, you’re less likely to face unexpected problems or setbacks further down the line.
Feasibility studies also represent the first touch point with real people that could be involved in the research. This allows the target group to be the central focus and understand what works for them. This opens up the opportunity for researchers, clinicians, and participants to collaborate and learn how best to conduct the study.
Funding pilot and feasibility studies
Once you’ve got the findings from your feasibility trial, it’s going to be much easier to progress to running the actual trial, because you’ve rehearsed it. Not only that, but it will also help secure the funding needed to run the bigger trial. After all, they’re not cheap. Being able to show pilot or feasibility data to funders proves that you’re coming to them with a tried and tested plan, boosting the chances that the main trial will be achievable.
That’s why at World Cancer Research Fund International, we offer specific grants for pilot and feasibility studies, as part of our Regular Grant Programme. These are for shorter time periods, with lower budgets than our investigator initiated grants.
Sometimes they prove to work well and achieve the intended results.

Dr Campbell
One example is our grant holder Dr John Campbell, who ran a pilot trial to assess whether a 16-week exercise programme for people with chronic lymphocytic leukaemia (a type of rare cancer of the blood and bone marrow) was safe and acceptable.
The study concluded that the programme was both safe and feasible, and even showed an increase in muscle mass and reductions in fat around the lower body.
Dr Campbell and his team also received positive feedback from the participants in the study, with one saying:
“I have strong memories of the trial. It came into my life during some dark days and gave me a sense of routine and a newfound purpose. I’m so grateful for the opportunity to meet the researchers, though I wish it had been under different circumstances.”
Dr Campbell and his team now plan to use this small-scale study to inform a larger trial that will, for the first time, assess the tumour-suppressing effects and mechanisms of exercise in chronic lymphocytic leukaemia.
Sometimes pilot studies can highlight challenges and important considerations for a study’s design. And these results are just as important.
Not only does this save a lot of time and money on a trial that won’t succeed, but it’s also an essential way to learn what doesn’t work, so other researchers can avoid encountering the same issues.

Prof Craike
Take, for example, a project led by grant-holder Prof Melinda Craike and funded by our network charity Wereld Kanker Onderzoek Funds. The study examined the feasibility of a nurse-delivered physical activity promotion intervention for prostate cancer survivors living in socio-economically disadvantaged areas. Recruitment was low, and both nurses and survivors reported only low to moderate acceptability. Survivors highlighted barriers such as a lack of interest, perceived cost, other health concerns, and a preference for advice from their general practitioners.
Rather than going ahead with a costly full-scale trial, Prof Craike and her team concluded the intervention was not feasible in its current form. Importantly, they also offered guidance for future research, such as exploring incentives for participation, involving GPs in delivery, and using community-based participatory approaches.
Prof Craike explains:
Pilot and feasibility studies might not always produce the results researchers expect, but they always offer valuable insights. I encourage the publication of feasibility studies, including those that are unsuccessful, to reduce waste and duplication, and to inform the development of future research efforts. Even though they are often unpublished, reporting unsuccessful feasibility studies like ours is essential to protecting research resources and guiding future projects.
Far from being ‘failures’, pilot and feasibility studies are crucial for developing smarter, more sustainable research.
Latest blogs
Why are we thinking about the food of the 1990s? Well, 3 decades ago, we funded an exciting project on women’s health. Now, 30 years later, scientists and women from the study have gathered to look back on what the UK Women’s Cohort Study has achieved.
It’s an incredible moment for us because many research projects only last a couple of years. Such a long-term project can provide scientists with richer, more detailed information to help prevent cancer.
Read more


The UK Women’s Cohort Study (UKWCS), which we provided initial funding for, recently celebrated its 30th anniversary! This is an incredible achievement because many research projects only last a couple of years. Such a long-term project can provide scientists with richer, more detailed information to help prevent cancer.
The UKWCS, led by Prof Janet Cade from the School of Food Science and Nutrition at the University of Leeds, is one of the largest cohort studies investigating diet and cancer in the UK, comprising over 35,000 middle-aged women and representing a wide range of different eating patterns, which can help scientists research what protects against cancer and coronary heart disease. Participants are regularly followed up to examine what effect food and nutrient intakes have on their long-term health.
Preventing cancer through what we eat
The first survey was funded by World Cancer Research Fund and the data produced from this survey and later ones has been used to investigate:
- meat and fibre intake and breast cancer
- vitamin C supplementation and breast cancer
- fibre intake in type 2 diabetes and cardiovascular disease
Over 3 decades, these investigations have provided interesting findings. For example, women who eat more fibre have a lower risk of stroke, and women who eat more red and processed meat have a greater risk of developing breast cancer.
Of course, we do not eat specific nutrients alone, so dietary patterns have also been identified and explored. Compared with meat eaters, vegetarians and fish-eaters (non meat-eaters who do eat fish) may have some protection against post-menopausal breast cancer.
This wide-ranging set of data can be used to identify common trends and to help target health information. For instance, women who eat more fruit and vegetables tend to be vegetarian or vegan, to take vitamin or mineral supplements, to be married, to be non-smokers, and to be educated to at least A-level or degree level.
To celebrate the milestone, World Cancer Research Fund hosted a party for colleagues who have worked with UKWCS over the last 30 years, in person and online from all over the country. Prof Cade talked about the UKWCS, and gave us some reminders of how different the world was 30 years ago. Diet is complex, so we need to understand how various factors interact to influence our health. It was fantastic to hear about all the findings so far from the project, and see so many people in the room who could share memories of working together.
Dr Darren Greenwood shared some reflections about the history of the UKWCS and its origins, from when we awarded the University of Leeds funding to investigate links between diet and cancers. The UKWCS grew and grew as more researchers worked with the data, and were awarded further funding. Sadly some members of the original cohort have died since the study launched. Yet Dr Greenwood reminded us that this data tells a story that helps us decode how to prevent cancer, and help people live longer, healthier lives.
This legacy is one of the enduring strengths of the UKWCS. The study has been cited in at least 9 government policy documents, providing direct life-changing information to help improve health and lives on a population scale.
Dr Diane Threapleton is one of the researchers who has used UKWCS data, including looking at how increasing fruit and vegetable intake slows weight gain. She focussed on the women of the study, highlighting how the data, time and samples they provided open a vital window into how what we eat interacts with real life. This was a timely reminder of the contributions of the women of the study, without whom none of this would have been possible.
Insights into ageing and beyond
After this, we heard from Yuanyuan Dong, who is working with the UKWCS to examine how diet affects the risk of rheumatoid arthritis. Yuanyuan joined us online from China, highlighting the global reach of the experts working with the cohort.
Finally, Dr Sarah Jing Guo told us about her plans for the UKWCS data – looking to the next 30 years! She gave us details of what her PhD student, Xinyue Liu, is examining with her project looking into how replacing processed meat with unprocessed meat or dairy products affects the risk of developing type 2 diabetes. She also gave us insights into how the cohort data could aid research into an ageing population, looking at Parkinson’s disease, Alzheimer’s or musculoskeletal disorders.
This amazing piece of long-term research is an important reminder of how small seeds of funding can have an impact over many decades and even lifetimes. We’re truly grateful to the donors of 30 years ago who helped make this research happen.
> More details about the UK Women’s Cohort Study, including information about publications

Documents from the UK Women’s Cohort Study

Help us fund the research of the future
Gifts in Wills help us fund long-term research projects like Prof Cade’s
 We spoke to Dr Renate Winkels (pictured) and Dr Laura Winkens, at Wageningen University & Research, to discover more about their studies in bowel (also known as colorectal) cancer.
We spoke to Dr Renate Winkels (pictured) and Dr Laura Winkens, at Wageningen University & Research, to discover more about their studies in bowel (also known as colorectal) cancer.
Your team looked at what influences people’s health behaviours after they’ve been treated for bowel cancer. What do you mean by health behaviours and what did you find out?
Health behaviours are the everyday choices people make that affect their health. In this study, we focused on 2 things:
- healthy eating (more fruit, vegetables, whole grains and beans; and less fast food, red meat, processed meat, sugary drinks and alcohol)
- physical activity
For people who’ve had bowel cancer, healthy behaviour may be associated with living longer, feeling better and having fewer problems like fatigue.
However, in previous studies, we found that many bowel cancer survivors don’t make big changes after treatment. Survivors are dealing with side-effects from the cancer or its treatment (such as gastrointestinal problems, fatigue or body image distress), which can make it hard to eat well and stay active.
Our study looked at what helps or gets in the way of healthy behaviour for people who have finished treatment for bowel cancer. We found:
Personal factors matter
How much time people have, their motivation, what they believe about healthy habits, what they know, and the skills they have can all influence whether they eat well and stay active.
Support helps
Encouragement and support from family and friends, or feeling like healthy habits are normal in their social circle, can make a big difference.
Environment plays a role
Access to gyms, parks, or even just good weather can affect how easy it is to be active.
Cancer symptoms can get in the way
Ongoing physical issues after cancer treatment, like fatigue or bowel problems, often make it harder for people to stick to healthy habits. But if someone is feeling physically well, they’re more likely to eat better and stay active.
Mental health may be important
Depression or being unhappy with one’s body seem to be linked with less healthy behaviour.
In short, to help people with bowel cancer lead healthier lives after treatment, we need to focus on motivation, knowledge, support, and overcoming the challenges they face physically and emotionally.
Towards a more complete picture
Your team conducted a “systematic review”. What is that and why is it important?
We wanted to find out what other scientists had studied, so we could build our study on the latest evidence. Moreover, we wanted to provide an overview of the topic. We looked at 21 papers, but we started with around 800 publications, and had to sift through them to identify the relevant ones.
You divided the studies into quantitative or qualitative. Why did you choose to look at both?
Quantitative studies collected a lot of numbers and measurements. The studies used standardised questionnaires to collect data on dietary intake and other aspects of lifestyle. Those studies answer questions like “how many” or “how much”.
Qualitative studies focus more on experiences. Such studies are mostly interviews to better understand why people do what they do, or how people behave.
Together, they provide a richer, more complete picture of the challenges and motivations colorectal cancer survivors face.
Were you surprised that people find it hard to change their behaviour?
Not really. Most people will recognise how challenging it can be to always make healthy choices. After cancer, when you’re rebuilding your life, that can be even harder.
How important is mental health for people living with and beyond bowel cancer?
Mental health is a very broad topic. People who have had bowel cancer may have a stoma, or be suffering from fatigue, or from bowel functioning problems. These can have a real impact on your life, and it’s important to address them. Some care teams really have an eye on this, but it’s not always the case. One patient told me that she did not dare to discuss her feelings of severe fatigue with her oncologist, as the oncologist told her that “fatigue was not a thing” for people with bowel cancer. We need more awareness and integrated care that addresses both mental and physical health to truly support survivors’ wellbeing.
You’ve also looked at whether following our Cancer Prevention Recommendations can reduce fatigue for people with bowel cancer.
We set up a study to assess whether following the Recommendations would help people to feel less fatigue. Cancer-related fatigue is a symptom that many bowel cancer patients experience during treatment and after completion. What is disturbing is that this type of persistent, overwhelming sense of physical, emotional or mental fatigue is not proportional to activity nor relieved by resting or sleeping.
We recruited participants for the trial who were experiencing cancer-related fatigue. In a randomised study, half of the group received lifestyle coaching to improve their adherence to the Recommendations, while the control group did not.
The coaching really helped the participants to adopt a healthier lifestyle: over time, this group reported eating more fruit and vegetables, and less processed meat and sugar-sweetened beverages. Also, physical activity levels went up more in the group that received coaching than in the control group.
Nevertheless, those changes didn’t result in less fatigue. This suggests that while these changes have many benefits, managing fatigue may require additional, targeted interventions.
This grant was funded by Wereld Kanker Onderzoek Fonds based in the Netherlands, as part of the World Cancer Research Fund International network.
Key takeaways:
- The CO21 CHALLENGE Trial found that a structured exercise programme after chemotherapy led to a 28% lower risk of cancer recurrence in colon cancer survivors compared with usual care.
- This is the first randomised controlled trial (RCT) to show that exercise directly improves survival in colon cancer patients. It confirms what observational studies have long suggested.
- The results were presented at a recent conference and made headline news. Experts say the CHALLENGE Trial marks a shift from viewing exercise as a “nice to have” to a “need to have” in cancer care.
Colon (part of the large bowel) cancer survivors who took part in a 3-year structured exercise programme had a 28% lower risk of cancer recurrence or a 2nd cancer. They also had a 37% lower risk of death compared with usual care.
These findings were shared at the 2025 Association of Clinical Oncology (ASCO) Annual Meeting. They were also published in the New England Journal of Medicine.
The ASCO Annual Meeting is the world’s largest oncology conference. It attracts more than 40,000 attendees from around the world. Every year, ASCO highlights the latest advancement in treatments. It also shares the directions that have the greatest potential for progress and patient impact.
Spotlight on exercise
The CO21 CHALLENGE Trial pulled back the curtain on a weapon that has been hiding in plain sight: physical activity. The results of the trial showed improvement in disease-free survival and overall survival in colon cancer survivors in the aerobic exercise intervention group. This trial is the first gold standard RCT to show what has long been indicated from observational studies. This is a big deal!
The impact of exercise on cancer outcomes has been a topic of great debate. Observational research has shown improvements in survival and quality of life linked to higher levels of physical activity. However, observational study designs are limited. They do not show cause and effect.
Plus, they are hard to implement in clinical settings due to concerns that the reported effects may not truly reflect the impact of exercise (and may be due to something else).
Our research
Over the past few years, World Cancer Research Fund International has done extensive reviews through its flagship Global Cancer Update Programme (CUP Global).
CUP Global includes partnerships with American Institute for Cancer Research, World Cancer Research Fund in the UK and Wereld Kanker Onderzoek Fonds in the Netherlands.
Our CUP Global reviews look at the extent to which diet, nutrition and physical activity impact people after a diagnosis of breast and colorectal cancers with regard to:
- cancer-specific mortality
- all-cause mortality
- risk of cancer recurrence
- health-related quality of life
An expert panel judged the strength of this CUP Global evidence. There were some limitations. Still, detailed recommendations were made to strengthen future research. One of the key recommendations was for well-conducted trials to look at the impact of nutrition or physical activity. The CHALLENGE trial is therefore very timely.
The CUP Global analysis was published in the International Journal of Cancer. It was cited several times in the CHALLENGE trial manuscript.
The CUP Global analysis compared highest with lowest levels of activity. We found that all-cause mortality was reduced by 23–40% depending on physical activity exposure.
Prof Anne May, University Medical Centre, Utrecht
During our review of the literature concerning the impact of post-diagnosis physical activity on colorectal cancer prognosis for the Global Cancer Update Programme (CUP Global), we were unable to draw strong conclusions due to lacking evidence from randomized controlled trials. The Challenge trial provides exactly the evidence we were waiting for.
The summary estimate for studies that assessed activity dose was measured in MET hours per week.
- A 10 MET hour per week increase in activity was linked to a 24% reduction in all-cause mortality.
- A change of 10 MET hours per week was also the intervention goal in the CHALLENGE trial.
The effect sizes in this first, gold-standard RCT are remarkably well-aligned with the CUP Global analyses of observational studies.
During the presentation of the trial results at ASCO, the authors shared this chart. It includes the treatment benefits from approved therapies for colon, lung and breast cancer.
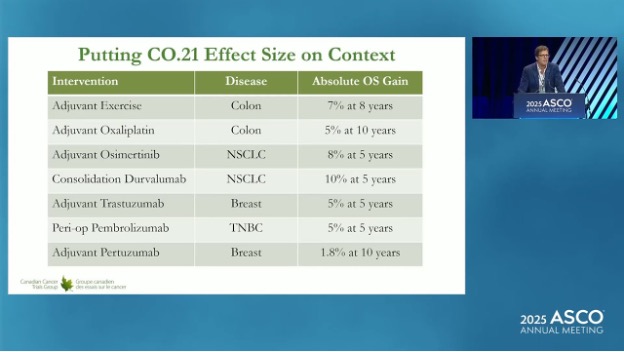
With 7–8% gains, you can see that exercise compares very favourably with other approved therapies in terms of absolute overall survival gain.
Collecting clinical trial evidence
The CHALLENGE trial confirms the clinical benefits that had been reported from observational studies. However, previous RCTs have also hinted at the accuracy of the results from observational studies. For example:
- The LEANer trial was published in 2023. It showed that triple negative breast cancer patients randomised to a diet and physical activity intervention before chemotherapy had a 53% higher rate of treatment success (eliminated cancer cells).
- A trial published in June 2025 showed that an exercise programme during and after chemotherapy increased the immune system responses in oesophageal cancer patients.
World Cancer Research Fund will fund the Optimus trial in the UK. Dr David Bartlett and Prof Adam Frampton at the University of Surrey will lead this study. It was proposed due to these findings.
Next steps
Dr Kerry Courneya co-led the CHALLENGE trial. At ASCO, he said these results could change practice for high-risk stage 2 and stage 3 colon cancer.
He expressed reservation that these results could be generalised to other sites and cancer stages. But he was optimistic that similar trials could be done more quickly than the CHALLENGE trial by taking advantage of newer methods. This could include using remote exercise assessments or activity trackers.
Dr Courneya noted that “support from funding agencies like WCRF/AICR is critical to moving this field forward because of limited access to funding for lifestyle research”.
AICR recently funded a project linked to the CHALLENGE Trial. It is led by Dr Kristin Campbell at the University of British Columbia in Canada. It will look at how muscle and fat tissue respond to exercise and how that may contribute to the observed survival benefits.
The response to the CHALLENGE Trial has made media headlines. Cancer researchers, doctors and patients are also excited by the news. This suggests that adding exercise as an additional part of treatment will gain further momentum.
While more trial data will be needed to support broader implementation, we are likely leaving the “nice to have” approach to exercise oncology and entering the “need to have” phase!
Research grants on physical activity
A selection of some of the grants we have funded that focus on the impact of physical activity on people living with and beyond a cancer diagnosis.
Latest news and blog posts

Prof Richard Cooke
Prof Richard Cooke is interested in what motivates people to drink alcohol – he surveys people to find out how psychological variables such as the intention to drink, attitudes about drinking, and regret after drinking alcohol – can predict how much people consume.
“Most of my research has been done with young adults aged 18–30,” says Prof Cooke, “because they were traditionally seen as the group that drinks the most, but this has changed in the last decade. I’m now doing much more research with middle-aged people. I also do studies assessing awareness of drinking guidelines, comparing how young adults and policymakers talk about alcohol, and reviewing the effectiveness of alcohol interventions.”
‘We know it’s dangerous’
“I find alcohol consumption fascinating to study as drinking has high social approval even though we know it’s dangerous. This means that health messages about alcohol are trickier to create than smoking messages. Saying ‘Don’t smoke’ is quite acceptable; saying ‘Don’t drink alcohol’ is less so,” he says.
Prof Cooke has several theories about why alcohol remains so popular across cultures: “Alcohol is a social lubricant: it relaxes people, makes them feel more confident and more able to socialise, especially with strangers. It’s really tied to our psychology in many different, sometimes unexpected, ways.”
A former student of Prof Cooke, Dr Joel Crawford, did his doctorate degree on regret and drinking. He asked young people adults about the fear of missing out (Fomo). When they don’t drink, some people think they are missing out on an enjoyable experience, like missing a party because you have to work. Dr Crawford found that the young adults would rather experience alcohol harms, such as hangovers and feeling sick, than miss events that heavily included alcohol, saying “Fomo was more painful to them than a hangover!”
This study illustrates the social and emotional barriers people trying to drink less may encounter. “It’s the social acceptability of drinking in most situations that makes it a challenge to reduce; drinking is associated with celebrations – birthdays, weddings, getting a new job, becoming a parent– and commiserations – missing out on promotion or the death of a loved one. Alcohol is also linked to healthy activities, like ending a walk in the countryside with a drink in a pub.”
Drinking’s a habit

“At the individual level, drinking habits are an issue. People develop habits when they perform the same behaviour in a stable setting, like drinking every Friday night in the pub with your friends. Breaking this habit means unpicking your routines in ways that people often don’t want to do.”
However, based on current trends, there will be fewer people drinking into middle-age and later life: “This has the potential to dramatically change how we organise events,” says Prof Cooke, comparing it to the rise in the availability and acceptability of non-dairy alternatives to milk. “People will be asking for non-alcoholic drinks at parties, and maybe that will become as acceptable as asking for an alcoholic drink is now.”
Young people prefer to stay in control
We asked Prof Cooke about why there is a decline in young people drinking alcohol. “There are several theories about why this is happening. One is that young people spend a lot of time online, and they want to present the best possible version of themselves as someone who is in control. Studies of Facebook content show that people generally share positive alcohol content, rather than negative experiences.
“Another idea is that alcohol has become more expensive in the last decade or so, which has put young people off drinking. Finally, the rise of energy drinks may be part of the explanation too, especially for young people who like to play games online. Energy drinks, high in caffeine, are likely to aid video game performance. Alcohol is unlikely to do this.”
For people of any age trying to limit their alcohol, Prof Cooke recommends trying to understand the reasons why you drink. “Do you drink to be sociable, to enhance an evening out, to cope with negative emotions? Are there other ways you could meet those needs? Psychological interventions, such as feedback on drinking or setting goals to drink less, can also be effective ways to cut back.”
Prof Cooke’s latest research
Prof Cooke’s latest research is published in Drug and Alcohol Review. He says: “Our new paper shows that policymakers and drinkers talk about drinking in different ways. While policymakers focused on drinking behaviour, drinkers talked about how drinking made them feel different emotions: embarrassed, happy, guilty, sad. Policymakers need to construct policies to reflect the importance of emotions in drinkers’ narratives.”
> Read the paper: The language of alcohol: Similarities and differences in how drinkers and policymakers frame alcohol consumption
Alcohol and cancer: let’s talk
In the UK, alcohol is a major part of how many of us socialise, relax, and celebrate. But do we really know the risks we’re taking when we drink?
Our research shows that most people don’t know that drinking any amount of alcohol increases the risk of 7 types of cancer.
This Cancer Prevention Action Week, we want to spark a national conversation: with friends, family – and within government – about alcohol and cancer.
Cancer Prevention Action Week
This year’s campaign focuses on the links between alcohol and cancer.