Courtney Bundrick will run for World Cancer Research Fund on 26 April 2026 to support cancer prevention research following the deaths of her parents.
The internal medicine physician, from Little Rock, is fundraising in memory of her mother – who died from ovarian cancer when Courtney was just 12 years old.
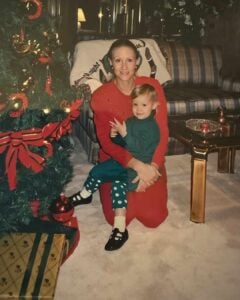
Courtney’s role caring for people with advanced cancer was also inspired by her father, who was a physician before passing away in 2023.
This frontline healthcare experience motivated Courtney to take action beyond hospital walls. By fundraising for cancer prevention research, she hopes to improve outcomes for future patients.
“Most of the cancer patients I see are either newly diagnosed with severe symptoms or suffering from advanced disease,” Courtney explained. “By that point, treatment options can be limited. That’s why I’m passionate about fundraising for life-changing cancer research.”
For Courtney, running has been a healthy release since medical school, and she has embraced discipline and mental resilience ever since.
“Training for a marathon takes months of commitment, but I love the structure and focus it gives me. It’s also a healthier way to manage stress, especially after starting my career during the pandemic.”

This dedication has not gone unnoticed by her patients, who are touched by Courtney’s efforts.
“Sometimes I’ll come into work after training, which often sparks conversations,” she shared. “Some of my patients were runners themselves, so it becomes a way for us to connect.”

World Cancer Research Fund CEO, Rachael Hutson, said:
“Every day, we see the impact that cancer has on people, families, and communities. It’s people like Courtney, who bring both professional experience and personal insight, that inspire change. By running the London Marathon, she’s driving forward life-changing research into how diet, nutrition, and physical activity can reduce cancer risk and improve survival. We’re grateful for her dedication and are incredibly proud to have her on the team.”
As she prepares for London, Courtney carries the memory of her mother and the stories of the patients she cares for every day.
“I’m doing this for them,” she said. “Anything we can do to advance research and prevent others from reaching the late stages, that’s what matters most.”
You can show Courtney your support by donating or sharing her story at the link below.
Read more supporter stories


Endorsement overview
The Continuing Professional Development (CPD) endorsement confirms the workshop meets high standards for evidence-based practice. It supports nutritionists and health professionals to maintain and build their knowledge and skills.
About the workshop
This 90-minute interactive workshop is based on evidence from our Third Expert Report on Diet, Nutrition, Physical Activity and Cancer. It turns research on cancer risk into practical, patient-centred guidance for health professionals to deliver to their communities.
The session covers key cancer risk factors including diet, physical activity, body weight, and alcohol. It also introduces WCRF’s 10 Cancer Prevention Recommendations.
Participants build confidence in discussing cancer prevention with patients and clients. The workshop explores common barriers and applies behaviour change techniques to support healthier habits.
Why it matters
Cancer prevention is a growing priority across healthcare systems as part of the NHS Long Term Plan. This endorsement highlights our role as a trusted provider of high-quality, accessible, and evidence-based training.
What the endorsement recognises
The Association of Nutrition highlighted that the workshop provides clear, relevant learning outcomes for nutrition professionals. It offers strong, evidence-based insights into how diet, nutrition, body weight, and physical activity affect cancer risk.
The live online format allows direct interaction with course leaders, while flexible delivery dates improve accessibility. Overall, it is a well-structured and valuable resource for continuing professional development.
Isobel Booth, Head of Health Information at World Cancer Research Fund, said:
In a time when misinformation about health and nutrition is widespread, it’s important that health professionals have access to credible, evidence-based information. Our workshops are grounded in robust scientific evidence and aim to support health professionals to have confident, practical conversations with patients about cancer prevention.
To find out more about the workshop and other resources, visit:
The latest news and blogs



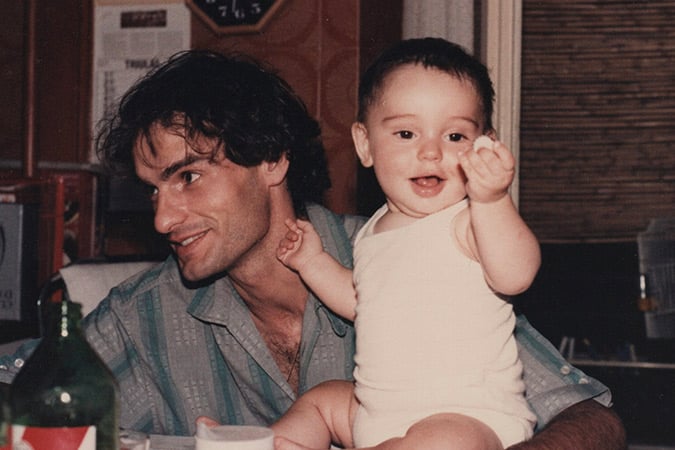
Riccardo Pilloni will take on the iconic event 22 years after his diagnosis and eight years after his father, Edmondo, died from liver cancer.
When Riccardo was 19 years old, he found a lump on his collarbone. He visited his GP and was told his symptoms could be seasonal flu related.
After his mother insisted that the doctor investigate further, Riccardo was referred to a haematologist. There, a biopsy revealed that this swollen lymph node was Hodgkin lymphoma – a type of blood cancer that begins in white blood cells.
“I remember feeling really healthy at the time, so the diagnosis was a huge shock,” Riccardo explained. “It felt like the rug has been pulled from under me.”
His treatment included chemotherapy followed by radiotherapy.
“When I looked in the mirror during treatment, I didn’t recognise myself. It destroys your body,” Riccardo shared.
Despite the long-term and late effects of his treatment, Riccardo considers himself “one of the lucky ones” having received an early diagnosis which meant his cancer had not spread. After months of treatment, he made a full recovery.
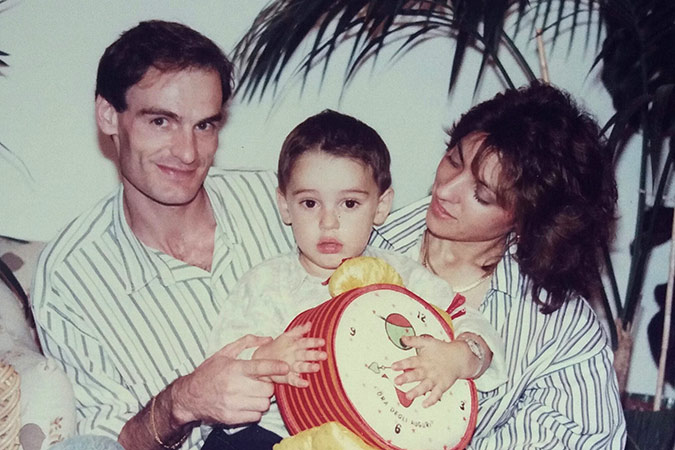
When his father was diagnosed with cancer years later, Riccardo felt a sense of helplessness as he watched him begin his own cancer journey.
“When I was fighting cancer, it was easier in a way because it was my own personal battle. But when it was happening to my dad, I felt powerless.”
After his father’s death, Riccardo became committed to supporting cancer prevention research and began his London Marathon training.
“Looking at how we can stop cancer before it starts feels like real progress. Trying to solve a problem like cancer before it begins, rather than treating it later, can save lives,” he added.
Riccardo says that grief and survival have shaped his outlook on life in equal measure.
“There is no finish line with grief, it stays with you forever. But when you’re going through cancer yourself, the finish line is going back to normal life,” he explained. “In both cases, you can’t see the finish line and you have to put the effort into moving forward.”

Running 26.2-miles through London is a personal commitment to honouring his dad’s memory and offering hope to others.
“I want people going through cancer to know that you’re not alone in this and there’s a beautiful life after.”
World Cancer Research Fund’s CEO, Rachael Hutson, said:
“We are incredibly grateful to Riccardo for turning such personal challenges into something positive. His experience, from a cancer diagnosis at such young age to the loss of his father, is the reality faced by so many families and shows why our work is so important. We will be cheering him on every step of the way.”
Now more than two decades in remission, Riccardo reflects both on the treatment that saved his life and the people behind it.
“I’m incredibly grateful to have survived and forever indebted to the healthcare professionals who treated me… and people I haven’t met too. Chemotherapy was developed and refined thanks to the tireless efforts of many scientists and I’m here today because of them.”
This gratitude is the driving force behind his fundraising efforts for World Cancer Research Fund.

“Now I’m focused on helping others. I’m taking on the London Marathon to help people diagnosed today who may not be as lucky as I was.”
You can show Riccardo your support by visiting the link below:
Read more supporter stories
The year is 2013. Macklemore and Katy Perry are on the charts. Children everywhere are about to lose their minds for Frozen. Most of the population has never even heard of a coronavirus.
In London, WCRF International’s recently established Policy & Public Affairs team has been hard at work developing the NOURISHING policy framework.
Following the success of NOURISHING, in 2018 the EU-funded CO-CREATE project enabled WCRF International to develop the MOVING policy framework and database, which outlined priority actions to promote physical activity.
Fast-forward to 2026, and we are now leading an exciting programme of work to update these tools: we envisage integrating policies on nutrition and physical activity into a single set of tools.
Alongside, we will incorporate policies on alcohol consumption and breastfeeding and infant nutrition to align with our current efforts to support population-level adherence to WCRF’s Cancer Prevention Recommendations.
As we embark on this project, we are reflecting on how our tools can drive policy action as effectively as possible.
How can our policy tools support action on prevention?
WCRF International designed the NOURISHING and MOVING tools to support our core policy aim: to help governments and policymakers around the world take effective action on preventing cancer and other non-communicable diseases (NCDs).
Since their publication, NOURISHING and MOVING have been cited hundreds of times in academic literature and referenced by national governments and organisations including the World Health Organization, the Food and Agriculture Organization and the Organisation for Economic Co-operation and Development. Their uptake has shown how these tools can support change across the policy process.
Policy frameworks provide a suite of actions to advocate for and implement. Given our focus on prevention, our frameworks have encompassed a whole-of-society and whole-of-government approach to supporting healthier populations, from retail environments, to urban planning, to marketing restrictions.
As well as providing policy options, policy frameworks can be used to monitor and benchmark policy progress. In 2023, our team used the NOURISHING and MOVING frameworks to carry out a benchmarking process in the European region, assessing progress on nutrition and physical activity in 30 countries.
By presenting the range of actions governments can take, policy frameworks provide a yardstick to identify countries’ strengths as well as priority areas for action.
The NOURISHING and MOVING frameworks were also used to guide the development of complementary policy databases. These databases catalogue real-world examples of policies from around the globe. For governments and advocates, learning from other nations’ experiences can be extremely valuable.
Consider sugar-sweetened beverage taxation, a policy measure which has now been implemented in over 100 countries, typically with the aim of reducing sugar consumption in the population.
A government looking to implement a sugar-sweetened beverage tax in their own context can learn from the example of Mexico, who implemented a flat excise tax of 1 peso per litre, or South Africa, who structured their tax based on sugar content.
They may be interested in knowing about the policy process that led to successful adoption in Chile, or how the measure impacted economic outcomes in the UK. Policy databases like NOURISHING and MOVING can help provide this information.
What’s next?
Over a decade after the launch of our first policy framework, the policy environment for prevention of cancer and other NCDs has evolved. Emerging issues such as ultra-processed foods, GLP-1s, climate change and air pollution are taking centre stage.
Governments are increasingly focused on policy integration and coherence in a bid to take effective action on complex issues. Advocates are exploring co-benefits and trade-offs with other agendas in order to build effective coalitions, particularly in the context of shrinking resources for public health.
Questions we are contemplating as we begin this project include:
- How can we best integrate a range of modifiable risk factors – nutrition, physical activity, alcohol consumption and breastfeeding – to reflect WCRF’s Cancer Prevention Recommendations?
- What types of information will be most valuable to our intended audiences, and how can we effectively mobilise these tools to support evidence-informed prevention policy?
- How should we navigate between depth and breadth in our database, weighing up the advantages of incorporating a wide range of policies from many countries, versus providing more detailed information around policy content, process and impact?
- How can we best incorporate co-benefits and trade-offs into our tools, acknowledging that actions that support cancer prevention can have synergies with agendas like climate change, health equity and mental health?
- Can our policy tools make space for and even drive innovation, as well as providing examples of precedent?
- How can we include country context in a way that helps our users understand what is likely to be feasible or effective in their own setting?
- What opportunities do AI innovations present for for expanding our coverage while maintaining the quality of our resources?
As we move forward with the next phase, we will engage experts and knowledge users in different regions and sectors to understand how we can best position these updated tools for use and take stock of the existing ecosystem of policy tools to ensure our work complements the efforts of other organisations.
If you would like to find out more about the policy framework and database update project, or see how you can get involved, please reach out to Chloe at c.cliffordastbury@wcrf.org.
More policy-related news and blogs



Marta Mixa is running the iconic TCS London Marathon for World Cancer Research Fund – earning all six stars from the original Abbot World Marathon Majors series (the world’s most prestigious long-distance running events).
Born in San Salvador and a US citizen for 40 years, Marta began her six-star journey back in 2019 with the New York City Marathon. After qualifying Boston and Chicago and running Berlin in the same year, Marta went on to complete three World Marathon Majors in 2022 alone.

In 2024, she crossed the finish line once more, completing the Tokyo Marathon and bringing herself one step closer to the iconic medal. Now more determined than ever to conquer the programme, Marta registered for the TCS London Marathon in a bid to earn her sixth and final star.

Fundraising for cancer prevention research is important to Marta after losing her aunt to breast cancer in 2024.
“She fought until the very end, but cancer stole her life, leaving three children, grandchildren, and her great grandchildren behind”, Marta shared. “It was really hard because she was the first family member that ever passed away from cancer.”
Marta’s sister-in-law, Sue, was also diagnosed with cancer in another devastating blow for the family.
“Sue was a vivacious, strong woman who loved the great outdoors and lit up every room. She fought for six long years and it was hard to see her go.”
Driven by her loss, Marta committed herself to not only support cancer research but to embracing a healthier lifestyle – which is proven by science to reduce risk of cancer along with many other conditions.

Marta’s love of running began in her late thirties, and over the past six years, she has completed 15 marathons. She credits her strength and endurance in her sixties to a balanced, nutrient-rich diet.
“The right protein is so important, together with carbohydrates. Carbs give you energy, and protein keeps you strong. I try to incorporate lots of fruit and vegetables into my diet, as well as lean protein such as salmon and chicken”, Marta explained.

World Cancer Research Fund’s UK Director, Steve Greenberg, commented:
“Marta is an unstoppable force, and her dedication to funding life-changing research is truly inspirational. Her active lifestyle and balanced diet echos our Cancer Prevention Recommendations, which help people live longer, healthier, and happier lives free from the devastating effects of cancer. She embodies everything that World Cancer Research Fund is about, and we are truly grateful for her support.”
For Marta, the journey has always been about more than medals.
“My motivation is letting others know they can do it too. Your age doesn’t matter”, she explained. “Stay strong, stay fit, stay healthy. Your body will thank you for it.”
You can show Marta your support by donating or sharing her story at the link below:
Read more supporter stories
Neuroendocrine cancers are a group of cancers that develop in cells of the neuroendocrine system. They can develop in different parts of the body such as the stomach, bowel, pancreas, or lungs.
Raine was just 17 years old when her father called her and her siblings with the news.
“It felt like the whole world changed in a second”, she said. “In the following months, I was wracked by fear and unpredictability about what the future held for mum and us.”
For years, Raine also worried the diagnosis might mean a higher risk for her too. Recently, she learned that it isn’t hereditary and her mum’s long-term outlook is encouraging.

Raine watched her mum bravely keep moving forward through her illness, including completing an MBA degree along the way.
“The experience has reshaped how I see health, time, and what’s possible. Every step I take when training is for those who can’t”, Raine shared. “Running the London Marathon is my way of honouring what my mum has been through and helps fund research so families can have more years together.”
In July 2025, Raine ran her first 5km in years. Since then, she has learned so much about the world of nutrition and eating healthier for training. This helped her to steadily increase her distance, recently completing a punishing 28km run.
On long training days, Raine’s dad often cycles alongside her in locations including Stellenbosch, surrounded by beautiful landscapes.

Raine has also started sharing her progress on social media, something she was initially nervous about.
“Don’t be scared to share your journey”, she said. “People really do want to back you.”
World Cancer Research Fund’s UK Director, Steve Greenberg, commented:
“We are so grateful to Raine for taking on the London Marathon in support of our vital work. Everyone here would like to wish Raine the best of luck as she takes on this incredible challenge in honour of her mum, all while raising awareness about the importance of cancer prevention research.”
Reflecting on her involvement with WCRF, Raine shared:
“I want to help people reduce cancer risk, including for cancers that receive less public attention.”

She’s asking supporters to donate, share her page, and help spread the word.
Read more supporter stories
The race will mark the halfway point in Val Aguilar’s effort to complete the original World Marathon Majors – a challenge in memory of her best friend who lost her life to brain cancer at just 18 years old.
The TCS London Marathon marks the third of Val’s six races, placing her midway through the series which also includes Tokyo, Boston, Berlin, Chicago, and New York.

In London, Val will be running for World Cancer Research Fund – a charity that examines how diet, nutrition, weight and physical activity affect risk of developing and surviving cancer
Val met Mary Katherine in the first year of high school where they formed a friendship that would last a lifetime.
“With her, everything felt like an adventure. Even the simplest or the silliest of things felt like the coolest thing to be doing,” Val shared.
Just four years later, in March 2009, Mary Katherine was diagnosed with an aggressive brain tumour. Despite doctors’ best efforts to save her life, she survived just 14 months after her diagnosis.
“Having such a special meaning behind my miles after losing a best friend to cancer makes each run a little bit easier, and each race experience a little bit sweeter,” Val explained.
Through years of training, international travel and physical challenges, Val is fundraising to support organisations committed to understanding, preventing, and treating cancer.

“When I’m racing, I think about who Mary Katherine would be now almost half our lives later. It makes me feel close to someone who I can no longer grow closer to,” she shared.
Val’s London Marathon bid for World Cancer Research Fund highlights the importance of evidence-based prevention strategies and global collaboration to reduce cancer risk.

World Cancer Research Fund’s UK Director, Steve Greenberg, commented:
“We are incredibly grateful to Val for her determination and dedication to supporting cancer research. Her efforts not only raise vital funds but also inspire others to take action in the fight against cancer. By completing the world’s most iconic marathons, Val has transformed her grief into action, proving that one person’s determination can help drive change.
Val hopes her story will encourage others to fundraise for cancer research, live healthier lives, and spark vital conversations about the importance of prevention.
You can show Val your support by donating or sharing her story below:
Read more supporter stories
Nicole Latini is running the TCS London Marathon this April after training in her native US – raising vital awareness and funds for World Cancer Research Fund on both sides of the Atlantic.
Her London Marathon bid began in 2022 after her dad, Alan Latini, died following a three-year battle with bowel cancer.

Following her dad’s diagnosis, Nicole became committed to transforming her health by losing over five stone (70lbs), running three half marathons, and ‘completely changing’ her diet and lifestyle to help reduce her own cancer risk.
Despite endless rounds of treatment including immunotherapy, chemotherapy, radiotherapy, surgery and clinical trials, Nicole’s dad faced his cancer with what she described as “gratitude and grace” before sadly passing away on 4 February 2022.
“Anyone who knew my father knew him as charismatic, witty, caring, loving, and someone who would do anything for his family. I miss my dad more with every passing day. Every milestone, holiday, and birthday is a reminder that he’s not here with us and should be.” Nicole added.
Nicole began running one week after her father’s death to cope with her grief, and soon set her sights on the 26.2-mile route to stop other families facing the same heartbreak.
“Running quickly became an instrumental part in coping, even though I was awful at it. Over time, I made it my goal to use my running through grief to give hope to others in honour of my dad,” she shared.
Reflecting on the challenge ahead, Nicole commented:
“Everyday, we have a choice to show up for our family, community and society. My dad showed up every single day for all of us. I’m choosing to train and show up everyday, even when I don’t want to, for him, for all those facing cancer, and for everyone experiencing grief.”
Running the London Marathon holds a special meaning for Nicole. She studied to become a vet in the city, often returning to the US for the holidays and staying close to her dad through regular video calls. He was determined to see her graduate, but heartbreakingly never made it to London.
World Cancer Research Fund’s UK Director, Steve Greenberg, added:
“We are in awe of Nicole’s commitment to improving outcomes for others in her father’s memory. Channelling her grief in a way that will offer hope to future generations is so selfless, and every step Nicole takes this April will make our vital work possible. We cannot wait to cheer her on and congratulate her at the finish line.”
You can show Nicole your support by donating or sharing her story at the link below:
Read more supporter stories
Rates of childhood obesity have increased from 4% to 20% over the past 50 years. From a cancer prevention perspective, this is worrying news: childhood obesity often continues into adulthood, and our work shows that excess body weight in adults is linked to at least 13 different types of cancer. What’s more, our research has shown that higher body weight in childhood, adolescence and young adulthood is linked to an increased risk of colorectal cancer in later life.
To maintain a healthy weight, children need more support to eat a nutritious diet. Policy can help foster systems and structures that make healthy diets easier and, for kids, schools are a great place to start.
The morning bell
My apartment in London overlooks a primary school attended by about 130 students. Waiting for my morning bus to WCRF’s offices, I see parents accompanying their children along the bustling road to the school gates. From a nutrition perspective, this particular route must feel a bit like running the gauntlet: a rotating billboard in view of the bus stop advertises burgers and fries, while every other business sells fast food. UNICEF’s Feeding Profit report, published last year, highlights this as a global problem.
To tackle the food environment around schools, several local authorities in the UK have chosen to restrict the opening of new fast food restaurants around schools. Cities such as Leeds and Manchester have opted to either reduce the number of new outlets near schools or prohibit them entirely.
Elsewhere in the world, governments have chosen to implement school-focused marketing restrictions. Latin American countries are leaders in this space, with countries like Chile and Mexico banning unhealthy foods from being advertised in schools. In 2021, the local congress in Lima, Peru went further, passing a law to prohibit the marketing of unhealthy foods within 200 metres of schools.
Lunchtime
From my own childhood in Canada, memories from the school cafeteria include slices of pizza, chocolate chip cookies and a freezer selling ice cream and popsicles. Although we occasionally managed to bargain for a few dollars for pizza, my parents worried that this menu wasn’t healthy enough. We mostly packed our own, a task added to already busy mornings.
Comparing notes with my partner who grew up in Sweden – where school lunches have been free for all children regardless of income for over 70 years – he remembers a self-service soup and salad bar to go with the daily mains. That didn’t stop students from complaining – tarragon fish day was particularly disliked. In high school, they would occasionally head over to the local pizzeria for lunch when their pocket money stretched to it.
Our memories reflect not only the cross-cutting appeal of pizza but the variation in school meals, even in high-income contexts. Until last year, Canada was still the only G7 country without a school food plan. However, we are not the only ones that have struggled to provide schoolchildren with nutritious lunches. Only 37% of school meal programs have an objective to prevent overweight and obesity, and wealthier countries are more likely to provide unhealthy foods.
Meanwhile, school food superstars like Brazil show us what can be done, successfully establishing legislation for coverage, quality, and procurement practices, emphasising local foods. In Japan, procurement policies also favour local producers, and pair school meals with food and nutrition education.
Recess
Beyond lunchtime, countries are developing innovative approaches to improving the quality of snacks sold on school premises. In Chile, a suite of policy measures aiming to reduce the consumption of foods high in calories, sugar, sodium or saturated fat has included banning their sale in schools. This has led to an impressive reduction in the sale of these unhealthy foods in school kiosks.
In January of this year, the World Health Organization published its new guideline providing evidence-based recommendations to support countries in creating healthy school food environments. This cites evidence from countries like Chile, as well as measures to directly provide children with healthy alternatives, like the European Union’s school scheme to support the distribution of milk, fruit and vegetables. Meanwhile, the School Meals Coalition, a global multi-partner initiative, facilitates country commitments to initiate or strengthen school food programmes, and fosters collaborations to support their efforts.
From the morning bell to lunchtime to recess, every part of the school day offers an opportunity to shape healthier futures. World Obesity Day calls on us to advocate for stronger food policy and equitable access to nutritious foods. If we get this right in schools, we don’t just change what children eat today – we help reduce their cancer risk tomorrow.
More policy-related news and blogs
Scott Molumby will run three marathons over three months in memory of his best friend, Dan Logan-Thomas, who sadly died in December 2025 after living with cancer for eight months.
Scott’s challenge began with double ultra marathon along the Tarka Trail in his home of North Devon – which starts in Ilfracombe and finishes in Dartmoor National Park on 28 February 2026.

Just four weeks later, on 28 March, Scott will run an ultra marathon across the snowcapped mountains of Snowdonia in his Native Wales. The route will begin on the north coast at Conwy and will see him head up and down sixteen of the highest mountains in the range – all of which are over 3,000 feet high.
Finally, Scott’s challenge will conclude with the iconic 26.2-mile TCS London Marathon on 26th April, marking 58 relentless days for World Cancer Research Fund in Dan’s memory.

After meeting at Swansea University, Scott and Dan struck up a close friendship which spanned multiple continents – with the pair living together in Wales, Australia, and New Zealand.
“Dan was such a happy-go-lucky guy.” Scott said. “He made his own luck because he was so positive, right until the very end.”
Over the last five years, Dan lived with multiple brain tumours which were non-cancerous (benign), undergoing multiple surgeries and radiotherapy while continuing to live a full and adventurous life. However, after losing feeling down his left side in April 2025, scans showed a new, large tumour.

Following major surgery, Dan received the devastating news it was cancerous, and began intensive chemotherapy which he faced with the same quiet courage that defined him:
“Dan wasn’t afraid of dying, he was more upset about how it would affect everyone else. That’s just the kind of person he was,” Scott shared.
Reflecting on the challenge ahead, which was once part of the plans they made together, Scott added:
“Dan helped me decide on the runs, and I always assumed he would join me at the finish line to celebrate. Now, I’m determined to complete this challenge in his memory and give it my all. It gives me an opportunity to remember a great friend in my own way with a lot of hard work, determination, and dedication.”

World Cancer Research Fund’s UK Director, Steve Greenberg, commented:
Taking on three marathons in three months shows Scott’s extraordinary strength and courage, and running in memory of his best friend is a reminder of the love and loyalty that shapes the best of us. His determination is raising funds to fuel our research that helps saves lives, continuing Dan’s proud legacy. We are deeply moved and profoundly grateful for Scott’s commitment to cancer prevention research.
For Scott, this challenge is about honouring the way Dan lived. He hopes that Dan’s story will inspire others to grab life with both hands.
“Don’t hang around if there’s something you want to do or something you need to say,” Scott said. Do it while you can, while you have the chance.”
You can show your Scott your support sharing his story or donating below:
Read more supporter stories
This could help many people stay healthy, as there are 3 million vegetarians in the UK and interest is growing in many parts of the world.
The research, led by scientists at Oxford Population Health’s Cancer Epidemiology Unit, pooled data from more than 1.8 million people across three continents through the Cancer Risk in Vegetarians Consortium – the largest ever study of non-meat diets and cancer risk.
They compared the risk of 17 different cancers across five diet groups: meat eaters, poultry eaters (do not eat red or processed meat), pescatarians (fish eaters), vegetarians (eat dairy and/or eggs), and vegans.
Compared with meat eaters, vegetarians had:
- 21% lower risk of pancreatic cancer
- 9% lower risk of breast cancer
- 12% lower risk of prostate cancer
- 28% lower risk of kidney cancer
- 31% lower risk of multiple myeloma.
However, vegetarians had:
- Nearly double the risk of squamous cell carcinoma of the oesophagus.
Tim Key
Dietary patterns that prioritise fruit, vegetables, and fibre-containing foods, and avoid processed meat, are recommended to reduce cancer risk. Our study helps to shed light on the benefits and risks associated with vegetarian diets.
Aurora Perez Cornago,
The higher risk of oesophageal squamous cell carcinoma in vegetarians and bowel cancer in vegans may relate to lower intakes of certain nutrients more abundant in animal foods. Additional research is needed to understand what is driving the differences in cancer risk found in our study
Dr Helen Croker
The results suggest non-meat diets are linked to lower risks for some cancers, though not all, highlighting important differences between cancer types and the role of different dietary patterns. To increase your overall protection from cancer, our advice is to build meals around wholegrains, pulses, fruit and vegetables, and avoid processed meat and limit red meat.
Yashvee Dunneram
Among the 72,000 vegetarians and vegans included in our study, the numbers of cases for some cancers were small, which limits the certainty of some findings. Moreover, nutrient intakes and overall diet quality vary substantially within and between vegetarian populations. Our next challenge is to collect more data on vegan diets and more data from other parts of the world.
There were no statistically-significant differences in risk for colorectal, stomach, liver, lung (in never smokers), endometrial, ovarian, mouth and pharynx, or bladder cancers, or non-Hodgkin lymphoma, leukaemia, and oesophageal adenocarcinoma in vegetarians.
Vegans had a statistically significant higher risk of colorectal (bowel) cancer when compared with meat eaters. For the other cancers studied, there was no evidence that risk in vegans differed from meat eaters, and for some less common cancers there were too few vegan cases to analyse. Further studies are needed to confirm these results in the vegan population.
Pescatarians had lower risks of breast and kidney cancers, as well as a lower risk of bowel cancer. Poultry eaters were found to have a lower risk of prostate cancer.
The full findings were published on 27 February 2026 in the British Journal of Cancer.
Latest news and blogs
World Cancer Research Fund’s Executive Director of Research and Policy, Dr Giota Mitrou, said: “On International Childhood Cancer Day, it is heartening to see global attention focused on the children and young people, and their loved ones, whose lives are changed by cancer.
We are proud to support studies that help us better understand how nutrition, physical activity and other lifestyle factors influence both risk and survivorship, and to ensure that childhood cancer remains firmly on the health agenda.
Each year, over 400,000 children and adolescents are diagnosed with cancer.
The rate of survival depends on the region. Children and young people with cancer have an 80% chance of survival in most High-Income Countries, but this drops to as low as 20% in Low- and Middle-Income Countries.
International Childhood Cancer Day is held on the 15 February each year. Childhood cancer affects individuals and families all year round, but the day itself provides a moment for us to raise awareness and develop a deeper understanding of the unique issues and challenges faced by those whose lives are touched by childhood cancer.
It also spotlights the need for more equitable and better access to treatment and care for all children with cancer, everywhere.
The World Health Organization (WHO) Global Childhood Cancer Initiative has a goal of increasing the survival rate of children with cancer to at least 60% by 2030, while reducing the suffering and improving the quality of life for all children living with cancer.
This goal can be achieved by increasing capacity to provide quality services for children with cancer around the world, and by prioritising childhood cancer at global, regional and national levels.
The recently-published National Cancer Plan for England places renewed emphasis on improving the nutritional care of children and young people undergoing cancer treatment, recognising that good nutrition is fundamental to treatment tolerance, recovery, and long‑term survival.
This focus on nutrition highlights the wider need for sustained research into childhood cancer that will strengthen our knowledge of how early‑life exposures, diet, physical activity, and environment shape both risk and survivorship.
Across the World Cancer Research Fund (WCRF) network of charities, we are funding studies that explore these factors and their impact on the lives of children and young people affected by cancer.
Using AI chatbots to support families of children with cancer
Dr Micah Skeens was funded by World Cancer Research Fund to test an AI powered chatbot called DAPHNE, designed to identify and manage the social and emotional needs of families caring for a child with cancer.
The research team found that the tool had high usability, and positive feedback from caregivers suggest that it can be an important resource is supporting families. By integrating AI technology into cancer care, it has the potential to revolutionise the identification and management of social needs in paediatric oncology.
Studying Burkitt lymphoma among children in sub-Saharan Africa
Dr Rita Khoueiry is funded by Wereld Kanker Onderzoek Fonds (WKOF) – our network charity in the Netherlands – to understand whether exposure to mycotoxins and infection with Epstein-Barr virus put children at risk of Burkitt lymphoma.
The research is exploring how in-utero and early-life exposure to mycotoxins (toxic compounds produced by fungi) may contribute, in combination with viruses and parasites, to the development of diseases such as Burkitt lymphoma, the most common childhood cancer in sub-Saharan Africa.
Understanding this relationship will set the foundation for developing new prevention strategies to protect at risk children.
Since food contamination with mycotoxins is expected to increase due to climate change, the results are of growing interest worldwide.
The FITco study: Can nutrition and exercise give children with cancer a better chance of survival?
Professor Wim Tissing and Dr Dieuwertje Kok are leading on FITco – a unique long-term study looking at body composition, nutritional intake and exercise in children with cancer.
The FITco study, launched in May 2025, is run by the Princess Máxima Center and Wageningen University & Research, and funded by WKOF.
FITco will follow 500 children newly diagnosed with cancer, tracking their diet, physical activity, and body composition. By understanding how these factors influence treatment, side‑effects, and long‑term health, the team aims to identify better ways to support children during and after cancer therapy.
With strong international collaborations, this research has the potential to shape global standards of supportive care in paediatric oncology.
Real-time tracking of environments and well‑being in young adults with cancer
Dr Katie Darabos is being funded by the American Institute for Cancer Research (AICR) to assess how aspects of the lived environment, and the movement of young adult cancer survivors, influences health behaviours.
Using GPS technology and real‑time surveys, Dr Darabos and team hope to understand how the environments young adults move through each day influence their stress levels, health behaviours, and overall well‑being.
By identifying the types of neighbourhoods or daily settings that increase stress or make healthy choices harder, this research will help pinpoint potential high‑risk environments.
The long‑term impact is significant – it could enable the development of targeted, mobile‑based interventions that support young cancer survivors exactly when and where they need it most.
Smart scans, stronger futures: AI and body composition in paediatric cancer survivorship
Funded by AICR, Dr Paul Yi is developing an AI‑powered tool to analyse routine CT scans and uncover how changes in body composition, such as muscle and fat levels, relate to treatment outcomes in children with cancer.
Right now, it is challenging to predict which survivors of childhood cancer will face serious health impacts down the line.
By revealing patterns that clinicians may not otherwise detect, the insights from this work could transform ongoing survivorship care. This research has the potential to help cancer survivors achieve better long-term health, reduce serious complications that often arise years later, and improve their quality of life.
Diet and exercise to improve treatment outcomes in B‑cell acute lymphoblastic leukaemia
Obesity contributes to the risk for developing acute lymphoblastic leukaemia. It is also known to increase the chance of chemotherapy being less effective and the disease returning in those being treated for it.
Dr Etan Orgel is testing whether targeted diet and physical activity interventions can reduce obesity risk during treatment for B‑cell acute lymphoblastic leukaemia.
This study, funded by AICR, has the potential to identify practical, evidence‑based strategies that make chemotherapy more effective and improve survival outcomes for children and adolescents living with this common childhood cancer.
Digital technologies to understand and improve physical activity in adolescents and young adults
Dr Lisa Schwartz is using innovative tools, including wearable activity monitors and real‑time surveys, to understand the daily factors that influence physical activity in adolescents and young adults with cancer.
By capturing the barriers that prevent young people from being active, this AICR funded research could pave the way for personalised interventions that help them overcome these challenges.
Ultimately, the aim of this research is to assist adolescents and young adults undergoing cancer treatment to be more physically active, which may ease their treatment symptoms and improve their mood and quality of life.