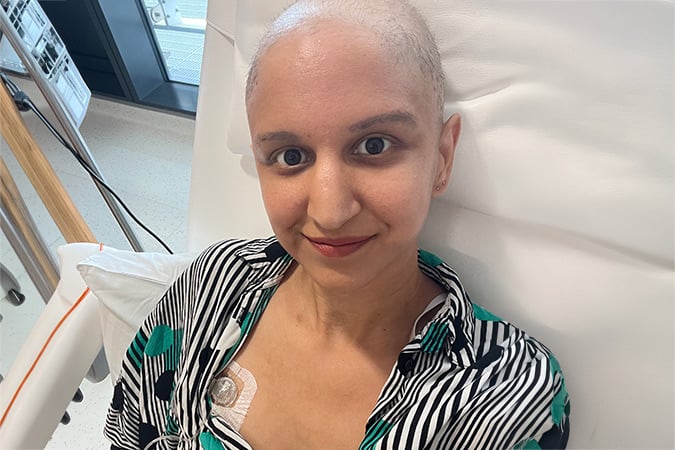
When her sister found a lump in her breast, Meera decided to get one of her own checked, which helped save her life. Now, she urges people to fundraise for research that could save others.

This July, Meera shares her story in support of our Jog 50 Miles in August challenge, which is fundraising for research into targeted treatments and improved advice and support for breast cancer patients.
While juggling life with two small children, Meera discovered a lump in her left breast which she believed was a blocked milk duct.

“I breastfed my son from birth. During this time, I noticed many lumps and bumps, so I just ignored it. Like lots of mums with young children, I didn’t think about my own health or prioritise it,” Meera said.
Months later, Meera’s sister found a lump in her own breast. After being checked and receiving the all-clear, Meera began to think differently about her symptoms.

Following a GP visit, Meera was sent for further tests. After scans and a biopsy, she was diagnosed with hormone receptor-positive (HR+) breast cancer in March 2025.
“It’s a reminder of why it’s so important to have these conversations with loved ones. My sister sharing her experience with me effectively saved my life,” Meera added.

Her treatment involved sixteen rounds of chemotherapy over five months, followed by surgery and twenty rounds of radiotherapy. Reflecting on her diagnosis and treatment, Meera shared:
“It was heartbreaking and a huge shock. My biggest fear was not being around to see my children grow up.”
Now in remission, Meera prioritises exercise to support her recovery, visiting the gym at least three times per week to improve her strength and fitness.
“My gym has a machine that calculates your body composition and carries out a strength test to help you lift heavier weights over time.
“When I first took a strength test in January, after nearly a year of cancer treatment, I had the strength of a 73-year-old. My latest test showed that I now have the strength of a 25-year-old! Seeing this transformation has been incredible, as exercise has become a huge part of my life post-treatment,” Meera shared.
Recently, a study we funded showed that following evidence-based lifestyle recommendations can support long-term health after a cancer diagnosis.
Regular physical activity can also help people maintain a healthy weight, and having less excess body fat can reduce risk of several cancers.

Rachael Huston, World Cancer Research Fund’s CEO, commented:
“We are incredibly grateful to Meera for sharing her experience, which shows how research into breast cancer treatments is changing lives and why it is needed now more than ever. We’re proud to be funding pioneering research at the University of Southampton, which is bringing us one step closer to kinder, more effective treatments for breast cancer patients.”
Supporting breast cancer research is important to Meera after she benefitted from ribociclib, a form of targeted therapy, following its introduction for primary breast cancer patients in February 2021.

“Research makes change happen. My biggest fear is dying while my children are young, and every breakthrough brings me closer to a future where that fear doesn’t become reality. People who fundraise may never meet the people they’re helping, but they give families like mine something priceless: hope and more time together,” Meera added.

By signing up to Jog 50 Miles in August, you can offer the gift of hope to people like Meera.
Read more supporter stories



Twenty years ago, researchers in Mexico set out to answer a question that could not be answered retrospectively: ‘How do lifestyle, reproductive and environmental factors shape women’s risk of cancer and other chronic diseases over time?’
“The only way to do that is to start off with a group of people who are free of the disease and wait until that disease occurs,” says Dr Martin Lajous, who directs the Mexican Teachers’ Cohort (MTC), now one of the largest long-term health studies in Latin America.
Since 2006, the MTC cohort has followed more than 115,000 women working in Mexico’s public education system, generating evidence on breast cancer, cardiometabolic disease, smoking, sugar-sweetened beverages, alcohol and other risk factors.
But building the cohort was only the first challenge. For years, the team worked to solve a persistent problem – how to identify new cancer cases in a country without a national cancer registry. The turning point came in 2019 when the problem was finally solved and, as Dr Lajous puts it, the MTC moved from being “a promise of a cancer cohort to a realisation of a cancer cohort”.
While there has been great change around the world, and in Mexico over the last 2 decades, from evolving technology to changing eating habits, collaboration has remained central to the mission of the MTC.
Long term partners
Funding to establish the Mexican Teachers’ Cohort began in 2006. Since then, the MTC has followed more than 115,000 women working in Mexico’s public education system. It generates evidence on breast cancer, heart disease, smoking, sugar-sweetened beverages, alcohol and other risk factors.
Collaboration has remained central to the mission of the MTC. “None of this would have been possible without AICR and WCRF, you believed in us,” says Dr Lajous. “And we are forever grateful for this sustained support.”
The partnership between the American Institute for Cancer Research, WCRF and MTC remains strong and ongoing. In 2020, AICR funded a grant for Dr Lajous to study lifestyle and breast cancer risk in a prospective study of Mexican women. In 2026, AICR funded a grant for Dr Lajous to study fibre, gut microbiome and colorectal cancer risk in a prospective study of Mexican women.
In May 2026, the WCRF International bursary helped Dr Lajous’ colleague Dr Liliana Gómez Flores Ramos, PhD, to attend the International Agency for Research on Cancer (IARC) conference in Lyon, France. At the IARC conference, she presented work on alcohol consumption and breast cancer from the MTC.
The story so far
The idea for the Mexican Teachers’ Cohort grew out of a 2004 case-control study on carbohydrates and breast cancer, led by Dr Isabel Romieu, Dr Walter Willett and Dr Mauricio Hernández. The study attracted wide attention, and inspired by international studies using teachers, sparked the idea for a prospective cohort based in Mexico.
Dr Lajous, who was based at the Harvard School of Public Health at the time, was invited to be part of the team setting up the project.
“We invited more than 115,000 women, working in the public education system in Mexico to provide us with details on their health conditions, but also on their lifestyle,” says Dr Lajous. “It was built with the intention of following up over time to be able to compare these lifestyle factors, or reproductive factors, in individuals who ended up having, for instance, breast cancer and those women who did not.”
From a promise to a realisation

ESMaestras researchers and operational staff at the Annual Liaison Meeting held on December 6, 2019, at the facilities of the Mexican Health Foundation (FUNSALUD).
When the cohort was first established, the program was able to collect baseline data. (such as age, menopause and smoking status, and BMI) and the participants have been completing questionnaires approximately every 4-6 years.
“But, in order to have a cancer cohort, you have to demonstrate that you can actually identify individuals who develop the disease,” says Dr Lajous. “And this element is what really took time to develop, making the primary challenge ascertaining incident cancer cases without a national cancer registry.”
By collaborating with different institutions in Mexico, the MTC were able to verify national IDs and have achieved approximately 97% ID coverage within the cohort. The national ID numbers then enabled cross-linkage with national mortality registries, cancer registries and health utilisation databases.
By 2019, they had developed a multi-source strategy to identify cancer cases using health utilisation databases (discharge data, consultations, medication use) from major healthcare providers.
“We dedicated three years to develop the method and convince the stakeholders, and to get everyone together, which took a lot of conviction, and then we finally got it done,” says Dr Lajous.“That’s when we went from being a promise of a cancer cohort to a realisation of a cancer cohort.”
Key milestones

An example of the questionnaire for participants, originally circulated by post.
Aside from officially becoming a cancer cohort in 2019, key milestones include findings that have had implications for prevention and public health policy.
Highlights include data on diabetes and weight gain that informed Mexico’s sugar-sweetened beverages tax. “Mexico has led efforts to change the dietary environment and reduce the consumption of sugar, sweetened beverages,” says Dr Lajous. “So, we conducted analysis on sugar-sweetened beverage intake and diabetes and also weight gain, which I think has been used by policy makers.”
The cohort has also produced some important work on smoking. “You may presume that we already know about the link between tobacco and cancer,” says Dr Lajous. “That may be so, but the pattern of tobacco smoking in Mexico, and particularly among women in Mexico, is one of occasional or very low consumption.
“There is a perception that if you only smoke a cigarette a week, it’s fine. However, we showed with the Mexican Teacher’s Cohort that even very low consumption of tobacco was associated with death.”
In recent years, external groups have begun seeking data from the MTC, shifting internal perception from a theoretical project to a strategic asset, something that Dr Lajous is proud of. “For the past 20 years, I’ve been reaching out to people to let them know how important the cohort is, how key this resource is, how they all should be proud of it. And now the dial has shifted, and institutions have started reaching out to us to collaborate, but it took time.”
Engagement and building trust
Teachers offered two advantages that made a long-term study feasible. Many were already used to completing written evaluations through an economic incentive programme, and their employment stability, healthcare access and pension system made it easier for researchers to remain in contact over many years. But the cohort’s longevity has depended on more than the suitability of teachers as a study population, it has also depended on trust.
“You must have a participant-centered approach, in the sense that if we promise something to the participants, be sure that you deliver that,” says Dr Lajous.
A key challenge for the team over time has been maintaining this engagement as teachers retire and communication has evolved from paper to electronic.
To ensure contact is kept consistent, the MTC plan monthly webinars, a well-attended series on health topics for all teachers, not just those who are part of the study. The team has also moved to home visits to collect data in-person for older, less tech-savvy participants. And, to ensure community building, created state-specific Facebook groups for participants.
Importantly, Dr Lajous stresses a two-way dialogue with the cohort. Feedback from teachers has helped shape the research agenda, leading to studies on stress and Adverse Childhood Experiences (ACEs). “One thing we’re always pushing for is that we keep our ears open to their concerns,” he says.
Lessons learned from the Mexican Teachers’ Cohort

Dr Martin Lajous speaking to the audience at the 20th anniversary event for the Mexican Teachers’ Cohort.
A lesson for Dr Lajous over the last 2 decades of setting up such a large-scale and long-term cohort is patience. “It’s a marathon in the sense that it requires consistency over time,” he says. “Understanding that this is a long-term investment and that you need to be patient. Sometimes things are not going great, but you just need to keep moving.”
People are at the heart of the project. Fostering a dedicated team and using international partnerships to build leverage and demonstrate value has been essential to the MTC. Dr Lajous also notes the importance of incorporating young investigators into the cohort and making them feel invested, so that the programme can be sustained over a long period of time.
“We are a relatively small team and collaboration with people outside of Mexico is important for us,” says Dr Lajous. “It gives us leverage in Mexico and also because it articulates that what we’re doing is important, and people elsewhere are seeing the value in the work that we’re doing.”
Future research
As the cohort enters its third decade, its research questions are changing with its participants.
“We want to understand the intersection between ageing, cognitive health, and cancer. So now we have a grant where we are going to visit 15,000-17,000 participants at their homes to perform in-depth cognitive assessments,” says Dr Lajous.
The team also plans to expand their work into environmental exposures including plastics, light at night, and climate-mediated events.
“And for me, the most salient cancer-related problem right now is colorectal cancer, which is increasing much more dramatically than other cancers. It’s currently the leading cause of cancer mortality in Mexico but we have very limited strategies for prevention and control of the disease.”
Reflecting on the last 20 years, Dr Lajous says, “I’m most proud of how this project has changed people’s lives and will potentially change a lot more people’s lives.”
Looking back, the cohort’s greatest achievement may be exactly what it set out to create – evidence rooted in real lives, sustained by trust, with the power to inform future generations on cancer prevention.
Latest news and blogs

A new study has identified five proteins in the blood that may help explain why people who are naturally ‘morning people’ tend to have a lower risk of breast cancer than ‘evening people’.
This work, led by researchers at the University of Hong Kong, was funded by Wereld Kanker Onderzoek Fonds, (WKOF) – the Netherlands-based charity within the World Cancer Research Fund network of charities.
The findings, published in the journal Communications Medicine, do not mean people can lower their risk simply by getting up earlier. Chronotype – our natural leaning towards mornings or evenings – is largely set by our genes and is hard to change. Instead, the real value of this research lies in the proteins themselves, which could point scientists towards new ways to prevent or treat breast cancer.
What is chronotype, and why does it matter for cancer risk?
Chronotype describes whether someone is naturally more of a ‘morning person’ or an ‘evening person’. Earlier research has linked having an evening chronotype, and other disruptions to the body’s internal clock – such as shift work, jet lag or irregular sleep – to a higher risk of breast cancer. But exactly why this happens has not been clear, which has made it hard to know what, if anything, could be done about it.
How did the researchers investigate this?
To dig into the biology behind the link, the team used a method called Mendelian randomisation. This uses genetic information to help work out whether one thing – in this case, chronotype – actually influences another, such as breast cancer risk, rather than the two simply appearing together by chance.
The researchers drew on genetic and health data from more than 650,000 people who took part in two large studies, UK Biobank and 23andMe, all of whom had self-reported whether they saw themselves as more of a morning or evening person.
They then took a two-step approach. First, they looked for links between chronotype and levels of nearly 5,000 different proteins in the blood, and found 895 proteins connected to a morning chronotype. Second, they checked whether any of those proteins were also linked to breast cancer risk and at this point, seven stood out as promising candidates.
To avoid false leads, the team ran an additional check called colocalisation. This statistical test shows whether the same genetic signal is genuinely influencing both the protein level and breast cancer risk, rather than two separate signals sitting close together by coincidence.
Dr April Shan Luo, Research Assistant Professor at Li Ka Shing Faculty of Medicine, the University of Hong Kong, who led the study, said:
“This gap in our understanding is significant in light of the growing prevalence of sleep deprivation in modern society and the challenges of being able to change or alter chronotype, particularly due to external factors such as shift work and frequent travel.
“There is a real need to better understand the link we are seeing between chronotype and breast cancer risk.”
What did they find?
After all the checks, five proteins stood out as having a genuine role in linking morning chronotype to a lower risk of breast cancer:
- ADAM15
- BTN2A1
- CASP8
- PDCD6
- RSPO3
Some proteins were more strongly linked to particular types of breast cancer than others. PDCD6, for example, showed the strongest connection to a subtype known as luminal A-like breast cancer.
Dr Luo, a recipient of the INSPIRE research grant, aimed at early career investigators, said: “We used large genetic datasets to examine morning preference, blood protein levels, and breast cancer risk. We also looked at different breast cancer subtypes and used breast cancer tissue data to assess the biological relevance of the proteins.”
Why does this matter?
World Cancer Research Fund International’s Assistant Director of Research and Policy, Dr Helen Croker, said:
“We know that there is a potential link between breast cancer risk and sleep chronotype, but this research has helped move the dial on our understanding of the biology behind this association.
The genetic tendency to be a morning person appears to be connected to a set of molecular switches, and some of those switches may also be linked to breast cancer risk. These findings improve our understanding of how sleep-related behaviour may influence breast cancer risk and further research could influence prevention strategies.”
Because chronotype is largely determined by our genes, this research is not a call to change your sleep habits. Its real potential lies in the proteins themselves: each one could be a possible new target for future cancer-prevention drugs or treatments, though that work is still at an early stage.
The researchers also note that their data came from people of European ancestry, so more research is needed to see whether the same proteins matter for people from other backgrounds.
Latest news and blogs
Today the Commons Health and Social Care Select Committee published a report on fixing the food environment as part of its food and weight management inquiry. Its message to Government is loud and clear: it is time to stand up to industry and move forward with a bold new approach to tackling obesity.
The environments in which we live, work and shop play a major role in shaping our health, yet many people are surrounded by the promotion and availability of unhealthy food options. Addressing this is essential for cancer prevention – excess weight is a cause of at least 13 types of cancer and is the second biggest preventable cause of cancer in the UK after smoking.
Many of the Committee’s recommendations are reflected in World Cancer Research Fund’s written evidence to the inquiry and, if implemented together, would help make the healthy choice the easy choice. In particular, we welcome the Committee’s recommendation that the healthy sales reporting policy should be introduced as soon as possible, with targets for major supermarkets set within the next 12 months and for the wider food industry by the end of Parliament. In practice, the policy would mean that large food businesses would be incentivised to have healthier products on their shelves and in promotions – leading to a potential reduction of obesity by around a fifth. We also strongly echo the Committee’s recommendation for the Government to exclude actors with a vested interest from discussions on the formation of policies on food, diet and obesity prevention.
Overall, the report sets out a clear roadmap for fixing our broken food environment. As the UK prepares for a new Prime Minister, we urge them to demonstrate their commitment to prevention by taking forward these recommendations at pace. This is a vital opportunity to fix our food environment, tackle obesity and prevent cancer for future generations.
Latest news and blogs
Cancer Prevention Action Week (CPAW) 2026 was a real success and a positive first step in what will be a three-year campaign. This year was very much about raising awareness of the scale and seriousness of health misinformation, particularly around nutrition, supplements, cancer prevention and cancer. As the campaign develops, we will be moving increasingly towards action.
Firstly, thank you to Alex Ruani, who worked with us to create the TRUST Test and supported the campaign through media, events and sharing the message with her networks. Thank you also to Dr Liz O’Riordan and Dr Philippa Kaye for their support throughout the development of the campaign, for acting as media spokespeople, appearing on radio and national TV, sharing across their networks and giving the campaign a platform at events.
We are especially grateful to Sharron Moffatt for so bravely sharing her story and calling out the scale and impact of health misinformation, particularly how difficult it can be to navigate after a cancer diagnosis.
We have already received some incredible feedback and will now test further to understand how it is perceived by the public, patients, and professionals. We would really value your feedback on it too, and would be grateful if you could take just 5 minutes to complete our survey.
During the week, we had more than 30 health professionals and experts backing the campaign, alongside organisations including the British Dietetic Association, the NIHR Cancer and Nutrition Collaboration, Patient Information Forum, International Agency for Research on Cancer (IARC), Our Future Health, Alcohol Change UK, Union for International Cancer Control (UICC), the Alcohol Health Alliance and the Obesity Health Alliance among many others.
We were also able to secure significant public and media engagement, including national press and powerful stories from people living with and beyond cancer, as well as support from MPs across their own channels. On 22 June, we also attended a roundtable on misinformation in the UK Parliament organised by author Deborah Cohen, which was another important moment in building momentum around this issue.
Cancer misinformation is an ongoing issue that we are taking very seriously. Together, we are stronger and together, we can help ensure people have access to information they can trust so that we can all live longer, healthier and happier lives free from the fear of cancer.


Latest news and blogs
Every day, millions of people search online for answers about cancer, diet and health. Some of what they find is accurate and helpful. Much of it is not. And when it comes to cancer – a subject where fear, hope and complexity are factors – misleading information can cause real harm.
Proving the challenge
There is no doubt that social media influencers promote a vast amount of misinformation online, especially to younger people. New YouGov polling, commissioned by World Cancer Research Fund for Cancer Prevention Action Week (15–21 June 2026), reveals a striking pattern:
- Among adults who rely on social media as their main news source, 13% wrongly believe that certain foods or diets can “starve” cancer, compared with 7% of other adults.
- 15% wrongly think certain supplements can reduce cancer risk, compared with 11% of other adults who prefer sources other than social media.
- Younger adults are particularly affected: 20% of 18–34-year-olds say they are more likely to trust a health claim if it is shared by an influencer or account they follow, compared with just 7% of over-55s.
Positive influencers speak out
However, there are also large numbers of influencers and experts online who are fighting back against misinformation. We are enormously grateful to the more than 30 health professionals and experts who gave their time to support Science Not Fiction — their commitment and expertise made a real difference.

Deborah Cohen
Deborah Cohen is one such expert. A medically-qualified journalist and author of “Bad Influence”, she warns:
“Over time, [influencers’] recommendations can start to feel less like advice from a stranger and more like guidance from a trusted friend.
They sometimes use scientific language to create an impression of authority, while the actual evidence behind their claims is weak, selective or simply not there.”
For anyone affected by cancer, the stakes are high.
Dr Idrees Mughal, known as Dr Idz, is a medical doctor with a master’s degree in nutritional research and more than 1.5 million followers across TikTok and Instagram.

Dr Idz
He explains:
“The danger is not just wasted money, but that misinformation can push people away from evidence-based advice and proven cancer treatments.
When people delay or reject effective care in favour of unproven alternatives, the consequences can be devastating, and in some cases fatal.”
Professor Sander van der Linden is Professor of Social Psychology at the University of Cambridge and author of FOOLPROOF.
He frames the broader challenge.

Professor Sander van der Linden
He says:
“Misinformation about cancer is rampant. One of the most important challenges is empowering people with skills to discern wellness quackery from evidence-based advice.”
The picture is not all bad online. The experts and influencers who joined us aren’t alone. Many doctors, dietitians, cancer specialists and science communicators are actively using social media to challenge misinformation with clear, evidence-based information.
How to tell the difference: the TRUST Test practical tool
That is exactly why World Cancer Research Fund has developed the TRUST Test – a simple, practical framework for evaluating health and nutrition information wherever you come across it. It gives you a clear set of prompts to help you pause and check before acting on a claim – whether you are reading a health blog, watching a video or seeing a claim shared in a group chat.
Join our campaign
Science Not Fiction is a three-year World Cancer Research Fund campaign tackling health misinformation and helping people find evidence-based information they can trust about cancer prevention, living with cancer, and nutrition.
Cancer Prevention Action Week 2026 was an important first step. The campaign reached a wide and influential audience, with backing from more than 30 health professionals and experts, support from organisations including the British Dietetic Association, IARC, Our Future Health and Alcohol Change UK, and coverage in national media.
You can be part of this work. Email us at pr@wcrf.org if you have a story to tell. You can also share the TRUST Test with friends, family or colleagues, and follow us on social media for reliable, evidence-based information about reducing your cancer risk and living with cancer.
Latest news and blogs
When Ben Wagenmann walked through a hospital radiation scanner and triggered every alarm in the corridor, it was not a malfunction. For several days after treatment, Ben is radioactive.
The 27-year-old medical AI student is living with metastatic cervical paraganglioma, a form of cancer so rare that only a handful of documented cases exist worldwide.
Ben’s original tumour developed around the fork of his carotid artery located in his neck. It measured around 5-6cm and required complex surgery lasting over ten hours to remove.

What makes Ben’s case so extraordinary is not only the tumour itself, but where the cancer has metastasised (spread). While cervical paraganglioma is typically benign (non-cancerous), Ben’s has spread throughout his spine, ribs and other bones.
Because no standard treatment exists, specialists across multiple hospitals in Europe worked on an experimental care plan. This included radionuclide treatment, a form of nuclear medicine requiring Ben to enter an underground radiation ward every six weeks.

“It genuinely felt like being in a bunker,” Ben said. “There were no door handles, and I couldn’t shower because it would turn the water radioactive.”
At one point, he triggered a hospital radiation detector simply by walking through the corridor.
“That was a surreal moment, realising you’re literally radioactive,” Ben added.

Following hospital discharge, Ben’s radiation levels were still so high that he could not be around pregnant women or small children safely.
Despite intensive treatment, regular hospital travel across Europe and the fragility of his spine, Ben has refused to give up the hobby he loves most – skiing.

“I’ve had to adapt. I’m more careful now and I notice the pain more, but skiing is one of the most important things in my life. I don’t want cancer to take that away,” he explained.
To raise awareness about cancer in young people, Ben began sharing his journey online through short ‘life recap reels’ on Instagram. Unexpectedly, the project raised hundreds of pounds for World Cancer Research Fund.
“I didn’t complete a marathon or jump out of a plane,” Ben said. “I just shared my life online and people connected with that.”
Rachael Hutson, World Cancer Research Fund CEO, commented:
“Ben’s commitment to sharing his journey is deeply moving, and we are grateful for the way he has turned his experience into hope for others. His fundraising efforts are helping fund life-saving research, and we are truly honoured to have his support.”
Following the success of his Instagram fundraiser, Ben completed a 16-kilometre race in his native Switzerland in May 2026 while on treatment break. He is now exploring a cycle across Norway to combine his love of endurance sport with fundraising.

Now, Ben hopes his story will challenge assumptions about what living with cancer looks like.
“You’re not just your diagnosis. Cancer changes things but it doesn’t automatically end your life,” he shared.
Ben shares his journey as part of our Every Step Tells a Story campaign.

Feeling inspired? Why not sign up to one of our exciting events and challenges today.
Read more supporter stories
When Sharron Moffatt was diagnosed with triple positive breast cancer in January 2024, her world was turned upside down. But alongside the physical and emotional toll of cancer, she faced another challenge: a flood of cancer misinformation.
The mental health first aid (MFHA) trainer and speaker, from Buckinghamshire, was working in the corporate wellbeing industry when she noticed her right breast growing in December 2023.

Sharron one day before her diagnosis with Rudy, the senior dog she adopted.
Just eighteen months earlier, Sharron’s mother died from metastatic breast cancer after facing the disease three times. It was this heartbreaking loss that prompted Sharron to always check her breasts.
“I miss my mum terribly, but I’m grateful to her because I learned so much about how to navigate cancer from watching her take it in her stride,” Sharron said.
Following tests at her local breast cancer clinic, Sharron was officially diagnosed with triple positive breast cancer on 7 January 2024.

A hospital selfie taken during one of Sharron’s tests.
Further investigations, including an ultrasound and biopsy, revealed three large tumours in her right breast which measured 12 centimetres combined.
“I broke down in tears wondering how I would tell my family, if anyone would ever work with me again and how I would walk the senior dog I adopted just one week prior,” Sharron shared.

Sharron with Rudy during cancer treatment.
Her treatment included seven rounds of chemotherapy, a single mastectomy and radiotherapy followed by further chemotherapy – spanning twenty months in total.
“Cancer takes so much from you, I was even on the cusp of having to stop treatment because I lost so much weight. During my first round of chemotherapy, I was really sick for around three days. When I finally recovered, it was time for my next infusion,” Sharron explained.
Despite the gruelling effects of her treatment, which included fatigue, hair loss, nausea and even liver cirrhosis – the hardest part of Sharron’s experience wasn’t the cancer itself. It was the misinformation that preyed on her through one of the most vulnerable moments of her life.
“During chemotherapy, I became so ill I didn’t recognise myself. That was hard. But the hardest thing for me, which still makes me uncomfortable to this day, was the misinformation I received,” Sharron said.
After sharing her cancer diagnosis on social media, Sharron was inundated with messages and claims about apricot kernels – the seeds found inside apricot stones – which were positioned to her as a “natural” cancer cure.

Sharron receiving an IV infusion.
The claims centre on a plant compound called amygdalin, which is found in apricot kernels, but there is no evidence that it treats cancer in humans. In fact, consuming apricot kernels can be dangerous because amygdalin releases cyanide in the body.
But the misleading claims didn’t end there. More recently, Sharron was contacted by someone on Instagram who claimed to have cured themselves of stage four melanoma by “healing their trauma.”
When Sharron asked for evidence to support the claim, she was met with defensiveness and hostility.
“Many of those on social media will deliberately target vulnerable people. I can understand why someone living with stage four cancer may be persuaded to try things like apricot kernels. However, they deserve access to reliable, evidence-based information that enables them to make informed choices about their treatment,” Sharron explained.
After completing her extended treatment plan in October 2025, Sharron continues long-term treatment (aromatase inhibitors). Following a meeting with her oncologist in May 2026, it was confirmed she currently has “no measurable evidence of disease” – marking an important milestone in her journey.

Sharron ringing the end of treatment bell with her identical twin sister, Lorraine.
Today, she dedicates herself to raising awareness about the dangers of misinformation and providing expert-led training on understanding cancer in the workplace.
“When you’re diagnosed with cancer, you’re dealing with fear and uncertainty. The last thing you need is misinformation adding to that. That’s why I’m passionate about encouraging people to know where to find trustworthy information and training employers on how to support people affected by cancer, including carers. No-one should have to face cancer and misinformation at the same time,” Sharron added.

Sharron today.
World Cancer Research Fund Head of Information, Isobel Booth, said:
“Unfortunately, Sharron’s story is not unique. Misinformation is seeping into more and more lives every day. This is why we are drawing attention to this important issue during Cancer Prevention Action Week. While we recognise there is valuable information out there, the science is often taken out of context, twisted or manipulated. For anyone affected by cancer who has questions on nutrition or supplements, please contact our Cancer and Nutrition Helpline, which is staffed by specialist oncology dieticians who can help filter through the noise.”
Sharron shares her story as part of World Cancer Research Fund’s Cancer Prevention Action Week campaign, which runs from 15-21 June 2026.
Latest news and blogs
This week, World Cancer Research Fund released new findings showing that 44% of patient-facing NHS staff encounter inaccurate or misleading information about nutrition and supplements at least once per week.
I am part of the 44%. Every week in my GP surgery, I see the consequences of health misinformation.
My patients arrive clutching newspaper stories, social media screenshots, printouts from wellness websites or saved videos from TikTok.
They are not reckless people, quite the opposite. They want better support for their treatment and to regain a sense of control.
Why “natural” doesn’t always mean safe
What worries me is not one miracle pill or herbal supplement. It’s the widely held belief that if something is sold over the counter, marked as “natural” or endorsed online, then it must automatically be safe. As doctors, we know that simply is not true.
Indeed, the full research for the action week shows that 42% of UK adults trust the health claims of products if they are legally sold in the UK.
There is also the dangerous assumption that “natural” means harmless, while prescribed medicines are somehow toxic. As I explain to patients, many of the medicines we rely on today originated from plants.
Nature can heal, but it can harm too. Doses matter, interactions matter and most of all, evidence matters.
Why health misinformation thrives online
In the digital age, separating evidence-based advice from misinformation has become extraordinarily difficult. We are bombarded with persuasive health claims, “life-changing” testimonials and confident voices that insist they have discovered what doctors do not want you to know.
I am incredibly cautious when someone is trying to sell certainty, especially when pushing a product.
Good doctors and other healthcare professionals do not make promises. We weigh up evidence, discuss risks and acknowledge the unknowns. Anyone claiming to hold “secret cures” or hidden truths should be approached with caution.
Because there is science and then there is science distorted, cherry-picked or stripped of context to put a price tag on hope.
Why false hope can be so powerful
This hope is a powerful currency. I know it not only as a doctor, but as a cancer patient myself.
When I was diagnosed with bowel cancer in my late thirties, I truly understood what vulnerability feels like. I would have done anything to get better, stay better and be with my children for longer.
People prey on this vulnerability.
The risks with supplements
As doctors, we talk about the importance of lifestyle factors because they matter: physical activity, diet, sleep, alcohol, weight. If I could prescribe exercise on the green prescription slip, I would.
On the contrary, the desire to improve our health can sometimes make us susceptible to oversimplified solutions or misleading claims. I have witnessed patients taking supplements that interfere with prescribed medication, or herbal remedies causing severe side effects on the skin and liver.
This is why it is so important to discuss any supplements, vitamins or alternative remedies with a healthcare professional.
You should never feel embarrassed about raising these conversations with your doctor. In my consultations, I want to make it as clear as possible: we are on the same team, and we both want you to get better.
Why questions are a good thing
No doctor knows everything; my patients teach me things every day. I have huge respect for informed for informed, curious people who ask questions and want to know more about their health.
In fact, I would trust a doctor who says “I don’t know, but let me find out” 100 times over one that claims to know all the answers.
How to spot health misinformation
When health information feels overwhelming or confusing, there are three simple steps you can take:
1. Pause before believing dramatic claims
Be sceptical of quick fixes, miracle cures and claims that sound too good to be true.
Take extra care if someone is selling a product alongside their advice.
2. Use trusted, evidence-based sources
Look for information from reputable organisations like World Cancer Research Fund.
They have developed a practical tool, called the TRUST Test, to help people assess health information before it causes harm.
3. Speak to a healthcare professional
You do not always have to speak to your GP.
Pharmacists, for example, are a valuable and accessible source of advice when it comes to medicine, supplements and the potential interactions between them.
Looking to a better future
Social media and the internet has transformed access to health information. At its best, it empowers people. At its worst, it leaves people vulnerable to exploitation, confusion and harm.
Good healthcare should never begin with fear or false promises. It should be built on honesty, evidence and trust.

Latest news and blogs
Health misinformation is widespread. Many people are still unaware that alcohol is a Group 1 carcinogen, linked to at least 7 different cancers including breast and bowel. This is unsurprising when you consider the alcohol industry’s long documented history of downplaying these well-established risks.
What’s more, alcohol is an outlier when it comes to labelling. Did you know that there is more legally required information on a bottle of water than on a bottle of alcohol? This is despite the serious harm alcohol can do, and the clear evidence that when it comes to cancer there is no safe level of alcohol consumption.
Cancer warnings on alcohol labels
To counter this and ensure people have access to clear, evidence-based information, World Cancer Research Fund (WCRF) and Balance are campaigning for a cancer warning to be included on the UK Government’s forthcoming mandatory alcohol labels, as outlined in our guest blog – It’s time to expose the great alcohol hoax. It is also imperative that industry-backed messaging such as ‘drink responsibly’ are removed, and that the policy is protected from industry influence more broadly.
The reality is that mandatory labels will take some time to come into force. In the meantime, WCRF has developed the TRUST Test, a simple tool to help people make sense of the health information they encounter online and separate fact from fiction. In our guest blog for Alcohol Change UK – Tackling persistent health misinformation on alcohol – we apply our TRUST Test to a common myth about red wine, showing how scientific research has been taken out of context.
Melissa Dando
The [red wine] myth originates from a study which found that a large amount of resveratrol, an antioxidant in the skin of purple and red grapes and therefore present in red wine, supported heart health in mice. The reality is that one would have to drink between 100 and 1,000 glasses of red wine a day to get anywhere near the amount of resveratrol equivalent to the doses that improved heart health in mice.
Health professionals also have a vital role to play. That’s why we’re calling for the upcoming NHS 10 Year Workforce Plan to provide additional staffing capacity and training on cancer prevention. This will help ensure that nurses and other patient-facing staff have the time and skills to counter the health misinformation, including on alcohol, that patients are increasingly bringing to their routine appointments.
Latest news and blogs
Despite widespread use of dietary supplements, research has shown that taking supplements does not reduce the risk of cancer. Instead, the strongest evidence continues to support following healthy lifestyle recommendations, including eating a balanced diet, maintaining a healthy weight and being physically active.
In our guest blog for MyNutriWeb, we explore common beliefs about supplements and cancer prevention, and highlight the challenges health professionals face when helping patients navigate conflicting nutrition information.
Why food comes first
While vitamins and minerals are essential for good health, experts recommend obtaining them through food wherever possible. Whole foods contain a complex mix of nutrients and other beneficial compounds that work together in ways supplements cannot replicate.
Rachel Clark
We recommend that people do not use supplements for cancer prevention. When it comes to cancer prevention, for most people, eating a healthy, balanced diet is more likely to help protect against cancer than taking dietary supplements.
Supporting informed conversations
With nutrition misinformation widely available online, health professionals have an important role in helping people understand what the evidence shows about supplements and cancer prevention.
The NutriWeb article provides practical insights to support evidence-based conversations and reinforces the importance of promoting healthy dietary patterns rather than relying on supplements.
What does reduce the risk of cancer?
While supplements do not prevent cancer, our cancer prevention guidance is grounded in decades of global research into diet, weight, physical activity and cancer.
We bring together the best available evidence to help people make informed choices – without hype or false promises.
Healthy dietary patterns, such as sustainable plant-based diets which prioritise vegetables, fruits, whole grains, legumes, nuts, and seeds, continue to show more consistent associations with cancer prevention than isolated supplements.
 Learn more
Learn more
To explore the evidence in more detail, join our webinar, Supplements versus food: What the evidence says about cancer prevention, which will examine the latest research and provide practical guidance for health professionals.

Latest news and blogs
One of the biggest health challenges of our time
Health misinformation is not a new challenge, but its scale and impact have increased significantly in recent years. At World Cancer Research Fund (WCRF), we are increasingly concerned about the ways in which misleading and inaccurate health information is hindering the public’s understanding of cancer risk, preventing cancer, and survivorship.
The rate at which misinformation is generated and disseminated has increased exponentially in recent years, driven primarily through increased use of social media and the rise of influencers, celebrities, and others sharing health advice online without formal scientific or medical training. This is having real-world consequences with attention diverted away from what we know reduces cancer risk, to promises of quick fixes and miracle cures.
That is why this year for Cancer Prevention Action Week (CPAW), we’re launching a three-year campaign to tackle health misinformation.
To kick off the campaign, CPAW 2026 will focus on sharing the latest evidence on cancer prevention relating to diet, supplements and alcohol. We will also raise awareness of trusted sources and promote WCRF’s practical guides that provide clear and up-to-date information people can incorporate into their daily lives.
In recognition that the issue of health misinformation is a systemic one, WCRF will also set out policy recommendations to address its causes over the course of the campaign. In 2026, these focus on supporting healthcare professionals to counter health misinformation, with future years likely to focus on addressing its causes.
Support for health professionals
Polling commissioned by WCRF highlights the burden health misinformation relating to cancer prevention and survivorship is placing on healthcare professionals. The forthcoming NHS Workforce Plan is a key opportunity to ease this burden.
First, the Plan must increase the number of patient-facing staff, such as general practice nurses, to improve patient access and allow time for conversations about cancer prevention during routine appointments.
Secondly, the Plan must help ensure that healthcare professionals are equipped with the latest information on nutrition, alcohol and physical activity as it relates to cancer. This can be done by embedding protected time for training within workforce planning. Crucially, the NHS Workforce Plan should also encourage education bodies to include cancer prevention and survivorship training in both pre-registration education and as part of continuing professional development (CPD).
The Plan must also recognise the ability to identify and respond to health misinformation as a core skill for patient-facing staff. Crucially, any increase in training must not simply add to existing pressures – instead training must be supported by additional staffing capacity and protected learning time.
Finally, there are many great resources on cancer prevention and survivorship that can support patient-facing healthcare professionals. For example, WCRF’s Alcohol and cancer: Let’s talk guide on how to have conversations with patients about alcohol and cancer can be particularly useful. Guides for the public, such as our 10 ways to protect yourself against cancer poster, provide clear, simple information that can support discussions with patients.
We also host a range of free, CPD certified webinars for health professionals, with one on supplements taking place on Wednesday 24 June – register for your place.
Addressing the drivers of health misinformation
While healthcare professionals have an important role to play in countering health misinformation, the responsibility does not rest solely with them. Instead, a broader, system-wide response is needed.
We know that around 40% of cancer cases in the UK are preventable. The evidence is clear: eating a healthy diet, maintaining a healthy weight, regular physical activity, and limiting alcohol reduce cancer risk. Yet online, this evidence competes daily with a vast and growing volume of content promoting fad diets, ‘anti-cancer’ supplements, detox regimens, and misleading claims about alcohol. Often commercially motivated and algorithmically amplified, this content frequently promises miracle cures and quick fixes.
The bottom line is that it’s unreasonable to expect people to navigate the overwhelming amount of health misinformation online without any safeguards. Currently, regulations in the UK permit ‘legal but harmful content’, which includes health misinformation. For example, an influencer promoting a supplement which they claim can cure cancer is producing content that is legal, despite it being harmful and untrue. This is unacceptable.
Algorithmic amplification then exacerbates the issue of legal but harmful content. A platform hosting misleading health content passively is one thing, but algorithms and paid advertising actively feeding it to people searching for health advice is more serious. While individual users should be held liable for what they post online, the platforms they post on should also be responsible, especially with regard to the systems they use to moderate, circulate and amplify content.
These are some of the challenges that we will be looking to address as our misinformation campaign develops. In the meantime, we have developed the TRUST Test, a simple tool that can help health professionals and their patients make sense of the health misinformation they encounter.
Join our Cancer Prevention Action Week campaign
Health misinformation online is not an issue that has arisen overnight and it will not be solved quickly, but Cancer Prevention Action Week (15-21 June) is a crucial start. Find out more about the campaign and how to get involved by visiting wcrf.org/CPAW2026.